

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- Each type of miscarriage or pregnancy complication listed below can be difficult, physically and emotionally.
- Understanding more about your specific type of miscarriage or pregnancy complicationcan help you make more informed decisions moving forward
- Most women go on to have successful pregnancies after a miscarrigae or pregnancy complication.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Early miscarriage vs late miscarriage vs stillbirths – the medical definitions
Threatened miscarriage
Inevitable miscarriage
Subchorionic hemorrhage
Chemical pregnancy
Blighted ovum
Missed miscarriage
Ectopic pregnancy
Recovering from a miscarriage
Going through pregnancy loss can be heartbreaking and confusing, so you may be seeking an explanation of what happened. In most cases, miscarriage happens due to reasons outside of your control, and couples do go on to have successful pregnancies after losses.
This article explains different terminologies and types of miscarriage so that you know what to expect, what treatment options are available, and when you can try again.
Early miscarriage vs late miscarriage vs stillbirths – the medical definitions
Miscarriages are pregnancy losses that occur before 20 weeks of gestation, which may affect 26% of all pregnancies and up to 10% of clinically recognized pregnancies.1 Early or first-trimester (before 13 weeks) miscarriages are medically different from late or second trimester miscarriages (weeks 14 – 20).
First-trimester losses, or early pregnancy loss, may affect about 10% of known pregnancies.2 Generally, there are fewer options to maintain the pregnancy during the first than the second trimester.
The most common causes for such early losses are chromosomal abnormalities or developmental problems. In such cases, there is no intervention that can save the pregnancy.3
Second-trimester losses happen between weeks 14 and 20. The chance of second-trimester losses is less than 1%.4 In cases of bleeding or other symptoms during the second trimester, there are more options to potentially maintain the pregnancy.
Stillbirths are losses that occur after 20 weeks.
Recurrent miscarriages or recurrent pregnancy loss (RPL) refers to couples with at least 2 – 3 miscarriages, which are not necessarily consecutive. It affects about 1 – 2% of couples trying to conceive and is medically different than spontaneous miscarriage. RPL could be due to ongoing hormonal, anatomic, genetic, environmental, infectious, thrombotic, or other unexplained causes.5 Therefore, couples with RPL should receive a thorough RPL workup to diagnose and treat the potential causes. In contrast, spontaneous or sporadic miscarriage may happen to any couple and tend to be a one-off loss without an ongoing cause.
In cases of threatened miscarriage, inevitable miscarriage, or subchorionic hematoma, the pregnancy is still ongoing but has become high-risk. It may be possible to maintain the pregnancy with different management strategies. In other cases, no intervention can save the pregnancy as the fetus has failed to develop normally.
Miscarriage may have no symptoms or present very differently, warranting different management for each patient.
Threatened miscarriage6
Threatened miscarriage is the most common complication of pregnancy. It occurs in about 20% of all pregnancies.
The main symptom of threatened miscarriage is vaginal bleeding that occurs before 20 weeks. After a threatened miscarriage, miscarriage is 2.5 times more likely, especially in women over 35 years old, with a history of previous loss, or low beta-human chorionic gonadotropin (βhCG). However, the pregnancy is still ongoing.
If you bleed during pregnancy, you should see your OB/GYN right away. They will evaluate the embryo and fetal heartbeat using a transvaginal ultrasound. The exam will look for signs of placental or subchorionic hematoma, a condition where blood collects around the placenta and may cause vaginal bleeding (see Subchorionic Hemorrhage below). The doctor will also check for cervical length and dilation.
Management of a threatened miscarriage both during the first and second trimesters may include:
- Bed rest
- Abstinence from sexual intercourse
For second-trimester threatened miscarriage, the doctor may recommend the following management methods:
- Cerclage, which is a stitch to hold the cervix together if the cervix is dilated, in case you have a history of cervical insufficiency that caused previous multiple second-trimester losses.
- Vaginal or oral Utrogestan, a progesterone medication that improves hormonal levels and endometrial receptivity.7
- Magnesium supplement to reduce cramping
Inevitable miscarriage89
Inevitable miscarriage refers to vaginal bleeding accompanied by cervix dilation. Although conception products haven’t passed yet, transvaginal ultrasound shows the tissue in the lower uterine segment or even in the cervical canal. In most cases, vaginal bleeding is heavier than spotting, and you can feel some cramping.
Without medical intervention, a miscarriage is unavoidable. However, in some second-trimester cases, there is a chance that the pregnancy may be saved.
For patients in the second trimester with inevitable miscarriage, management options may include:
- Broad-spectrum antibiotics in case an infection caused the inevitable miscarriage
- Progesterone
- Drugs that inhibit contractions, such as Nifelat
- Extreme anti-gravity bedrest
Generally, your doctor may try to maintain the pregnancy to viability at 23 weeks, which is the minimum age that the baby has a chance of surviving if it is delivered.
Subchorionic hemorrhage1011
Subchorionic hemorrhage or subchorionic hematoma (SCH) is one of the most common causes of vaginal bleeding. SCH is when blood collects between the placenta (and its outer layer chorion) and uterine wall.
Researchers still don’t fully understand the cause of SCH. However, it is more common in IVF pregnancies and those with recurrent miscarriage or uterine malformation.
The hematomas are usually small, leading to vaginal spotting. However, you should see your doctor and get an ultrasound evaluation with any amount of bleeding.
Typically, SCHs resolve by themselves, but most doctors will strongly suggest bed rest and abstinence, and some will even give progesterone. Usually, your OB/GYN will prescribe progesterone orally, vaginally through suppositories (if you have stopped bleeding), or intramuscularly, also referred to as progesterone in oil (PIO). The intramuscular injection has longer-lasting effects.
SCH is associated with an increased risk of early and late pregnancy loss, placental abruption, and premature rupture of membranes.12Therefore, even though it resolves naturally and should not be cause for concern, you should adhere to regular checkups if you’ve been diagnosed with SCH.
Chemical pregnancy
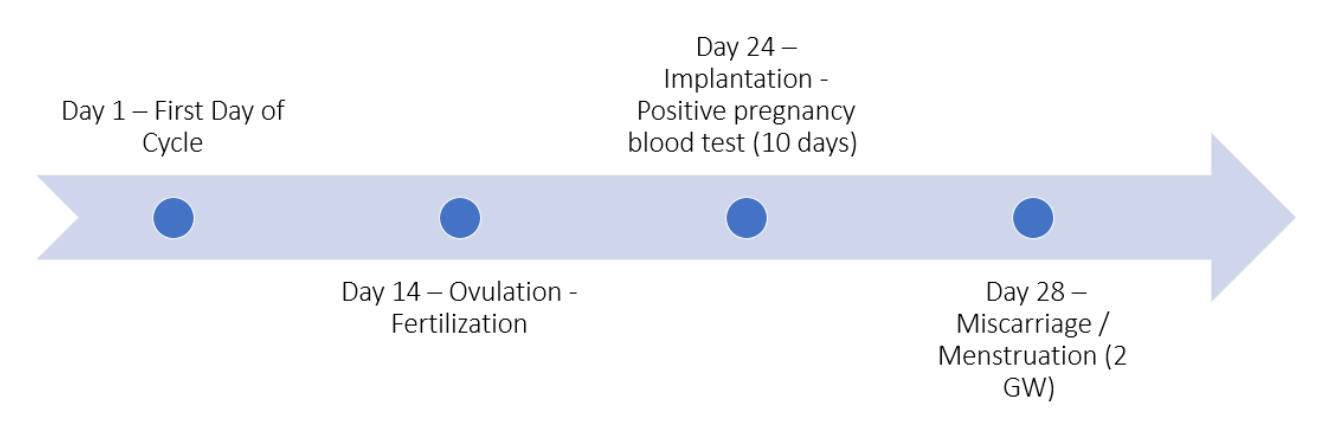
A chemical or biochemical pregnancy is a very early loss that happens shortly after the pregnancy becomes detectable by a sensitive pregnancy test, which is about 1 – 2 weeks after ovulation or 3 – 4 weeks pregnant. Chemical pregnancies may happen in up to 25% of all pregnancies and 50 – 75% of all miscarriages.13
Although chemical pregnancies happen during the very early stages of pregnancy, they are still considered a miscarriage and many couples grieve the loss.
Typically, an ultrasound can detect pregnancies after five weeks, so it will not detect a pregnancy before a chemical pregnancy occurs.14
It is unclear what exactly causes a chemical pregnancy. However, it is associated with endometrial abnormalities, chromosomal malformations, advanced maternal age, and sperm DNA damage.
After the embryo implants into the endometrium, pregnancy hormones increase. At this stage, the βHCG level is high enough for a positive pregnancy test but not for pregnancy symptoms. The bleeding may occur around the time of your period, so you may not even be aware that you are pregnant. Shortly afterward, the pregnancy is lost, causing the βhCG levels to drop and pregnancy tests to become negative.15
Blighted ovum16
Blighted ovum, or anembryonic pregnancy, happens when the gestational sac (a structure that develops after fertilization) is visible without a viable embryo.
Reasons behind blighted ovum are numerous and interconnected. They may include genetic factors such as chromosomal malformations, hormonal disturbances, and even infections. Read our blighted ovum article to learn more about potential causes.
At the beginning of pregnancy, the fertilized egg secretes βhCG that is detectable on sensitive pregnancy tests. The fetal pole, which is the proof of embryo presence, is visible from the 6th week on transvaginal ultrasound. If the pregnancy test is positive and no fetal pole is detectable on ultrasound past the 6th week, the doctor may diagnose a blighted ovum.
Usually, your doctor will tell you to wait another week and repeat the ultrasound to exclude the possibility of later implantation due to late ovulation. In addition, they will retest your βHCG to evaluate if gestation is indeed more than six weeks.
In a blighted ovum, there is no intervention that can maintain the pregnancy. Your doctor will counsel on available options to manage the miscarriage.
Missed miscarriage
In a missed or silent miscarriage, the fetal heart has stopped but the woman doesn’t experience any symptoms. The conception material stays in the womb even though the pregnancy is not viable. Sometimes there may be a brownish discharge or subsiding pregnancy symptoms.
A missed miscarriage is typically diagnosed with a transvaginal ultrasound checkup. Sometimes, the woman isn’t even aware she is pregnant and only finds out about the pregnancy during a routine checkup after a late period.
When the pregnancy is not viable, the conception material needs to be removed from the uterine cavity to prevent infections, sepsis, and dangerous blood clots. The three main options include:
- Expectant management, which involves waiting for the unviable pregnancy to resolve naturally
- Medical management, which requires medication, typically Mifepristone and Misoprostol, to resolve the pregnancy and expel the conception material
- Surgical procedures, such as a dilatation and curettage (D&C), which involves dilating the cervix and scraping to remove all the conception materials
The decision to resolve an unviable pregnancy is very personal and depends on a few medical factors. To learn more about these three options and how to decide which is best, see our miscarriage treatment options and D&C articles.
Ectopic pregnancy
An ectopic pregnancy occurs when the fertilized egg implants outside the womb. This type of pregnancy needs to be treated to prevent life-threatening complications. The standard treatment is methotrexate. However, if the ectopic pregnancy is further along or if the fallopian tube has ruptured, some patients may need laparoscopic surgery.
In an ectopic pregnancy, the fertilized egg may implant in the fallopian tubes, ovaries, abdominal cavity, or cervix. Causes of ectopic pregnancy may include endometriosis, previous uterine surgeries, pelvic inflammatory diseases, smoking, and advanced maternal age.
In a typical pregnancy, your OB/GYN will test your ꞵHCG and check for signs of pregnancy on the ultrasound, which becomes visible after 5 – 6 weeks. The ꞵHCG should double every 48 hours.
If the ꞵHCG doesn’t rise appropriately, your doctor may suspect an ectopic pregnancy. They will then confirm the diagnosis with a transvaginal ultrasound.
Sometimes, miscarriage symptoms may have already happened before the woman is aware she is pregnant. These may include bleeding, severe cramping, and tubal abortion, in which the conception material exits out the other end of the uterine tube.
In tubal pregnancies, the gestational tissues may invade the blood vessels in the fallopian tubes, causing severe internal bleeding. If this happens, an emergency laparoscopic or open surgery may be necessary to stop the bleeding.
Recovering from a miscarriage
While a miscarriage is both physically and emotionally painful, many couples find it takes longer to recover emotionally than physically.
Keep in mind that a miscarriage is not your fault. Take time to grieve and try again when you are ready. Physically, you will be ready to resume sexual intercourse and try to conceive after 1 – 3 menstrual cycles.17
If you’ve had more than two losses, you should be evaluated for potential causes of recurrent pregnancy losses. Sign up for our newsletter to get our lab test checklist.
For resources on moving on, check out our Moving Forward course and newsletter.
For 10 questions I ask before deciding on a D&C, read our D&C vs a natural miscarriage article.
In conclusion:
- There are different types of miscarriage situations, each requiring different management options.
- You may feel some symptoms or have no signs at all, and sometimes there is really nothing you or your doctor can do to maintain the pregnancy.
- It is not your fault.
- When you are ready, you can go through evaluations with your partner and decide when to start trying again.
Next Steps to Consider
- Determine what type of miscarriage or pregnancy complication you have experienced and talk to your doctor about treatment options.
- Depending on your situation, you may want to request additional testing and/or labwork, especially with recurrent or multiple miscarriages.
- Just because you are physically ready to move forward after miscarriage does not mean you are emotionally prepared and ready. Consider working with a therapist or other mental health practitioner. Take your time!
References

0 Comments