

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- Endometriosis is underdiagnosed and often overlooked
- While endometriosis is associated with infertility and miscarriage, women with endometriosis can conceive naturally
- There are specific treatment options that can improve endometriosis and reduce the risk of miscarriage
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Table of Contents
What is endometriosis?
Symptoms of endometriosis
Types and stages of endometriosis
What causes endometriosis?
How endometriosis affects pregnancy
Diagnosis of Endometriosis
Endometriosis treatments
Natural and experimental treatments
Endometriosis is a painful condition when your endometrial cells grow outside of the uterus. It can cause very painful periods, heavy menstrual flow, and pain during intercourse. Many women with endometriosis also struggle with infertility, pregnancy complications, and miscarriage.
Because it is under-recognized, poorly understood, and under-diagnosed, endometriosis is more prevalent than you think. It may affect up to 10% of premenopausal women and 30 – 50% of women who struggle with period symptoms, infertility, and pelvic pain 1. On average, it takes up to 6.7 years for women to be correctly diagnosed with endometriosis 2!
Although many women with endometriosis have had successful pregnancies, endometriosis does increase the risk of infertility and miscarriages 3. With this article, we hope to raise awareness, reduce diagnosis delay, and improve treatment outcomes by providing you everything you need to know about endometriosis.
What is endometriosis?
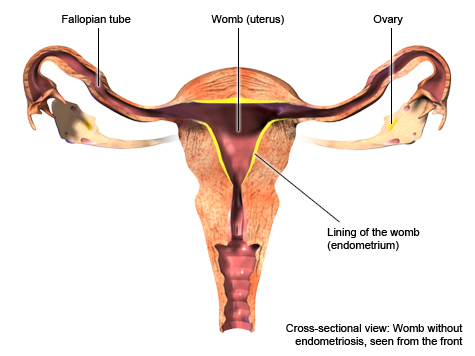
Endometriosis is an inflammatory and hormonal condition where endometrium-like tissues form lesions outside the uterus. The lesions could reside in the pelvis, around the uterus, in the Fallopian tubes, on the ovaries, and in the abdominal cavity.
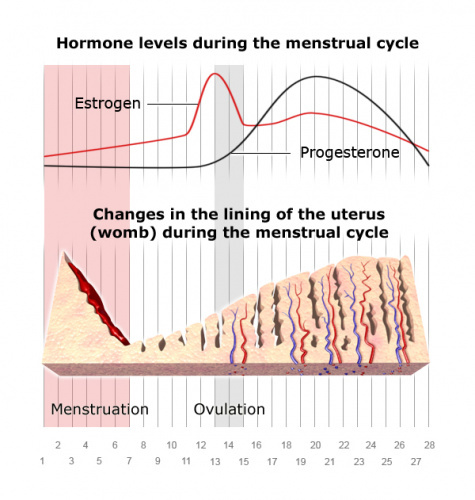
Normally, the endometrial tissue or endometrium line the inside of the uterus. Naturally, these cells respond to the ebbs and flows of hormones, including estrogen and progesterone, throughout your menstrual cycles.
Endometriotic lesions may grow and shrink with each cycle, causing severe menstrual pain. Depending on their locations, the lesions may also interfere with other bodily functions and fertility. Women with endometriosis may also have progesterone resistance both in their endometrium and lesion cells, contributing to pain and fertility problems 4.
Symptoms of endometriosis
There are no specific symptoms that indicate endometriosis. It presents differently in every case, so it is underdiagnosed and often overlooked for a long time. Many women with endometriosis, as detectable by a magnetic resonance imaging (MRI) scan, have no symptoms 7. Hormonal birth control may suppress endometriosis symptoms, so you may only experience these symptoms once you are off the birth control. Also, many endometriosis symptoms are easily confused with other conditions, such as irritable bowel syndrome and pelvic inflammatory diseases.
Common endometriosis symptoms include:
- Painful period with prolonged (>7 days) and heavy menstrual bleeding
- Anemia symptoms, such as fatigue, dizziness, and heartbeat 8
- Pain during sex 9
- Chronic pelvic pain 10
- Pain or abnormal function of the bowel or bladder, including constipation or diarrhea 1112
- Abnormal bleeding, such as from the rectum
- Other discomforts in the body, depending on the location of the lesions
The symptoms are often cyclical, recurring around the same time every month 1314.
Types and stages of endometriosis
There are multiple ways to categorize endometriosis. One is location-based, depending on where the endometriosis lesions are found, including:
- Peritoneal superficial endometriosis is considered the least severe form of endometriosis where the lesions attach to the peritoneum. The peritoneum is the thin membrane that lines the abdomen, abdominal organs, and pelvis.
- Ovarian endometriomas are a type of endometriosis that implant on or inside the ovaries.
- Deep infiltrating endometriosis invades the organs in the abdomen or pelvic cavity, causing scar tissue or obstructing their functions. These organs may include the ovaries, Fallopian tubes, gut, bladder, or rectum.
Endometriosis staging – The American Society of Reproductive Medicine categorizes endometriosis into four stages based on the number and depths of the lesions. These include minimal (stage I), mild (stage II), moderate (stage III) and severe (stage IV). The staging should predict the chance of a successful natural pregnancy, rather the degree of pain or other symptoms. Typically, your OB/GYN determines the endometriosis stage visually during a laparoscopic diagnostic surgery. However, many other factors could determine the extent of the disease, so some gynecologists are debating a more clinically useful classification 15.
What causes endometriosis?
We still don’t completely understand what causes endometriosis. There are many hypotheses about how it occurs, but none is universally accepted. These include:
- Samson’s Retrograde Menstruation theory, which says that endometrium-like cells travel backward into the pelvic cavity 16
- Cells that are outside the womb could transform into endometrial-like cells. These cells may have the same embryonic origin as the endometrial cells itself 17
- The endometrium-like cells travel into the pelvic cavity through the lymphatic system 18
Why we still don’t understand endometriosis
Currently, laparoscopy (keyhole) surgery is the only reliable way to diagnose and stage endometriosis. It is an invasive procedure that carries the risk and cost of surgery. This makes it difficult for researchers to study endometriosis or test treatments for endometriosis. Most endometriosis clinical trials measure pain or symptoms using questionnaires rather than repeating a laparoscopy.
Decades of research have attempted to find noninvasive lab tests that can screen for endometriosis, but there hasn’t been a medical consensus 1920. Therefore, it is difficult to identify the causes and treatments for endometriosis, especially when they need a large number of women to establish a medical consensus. However, we know a few risk factors of endometriosis.
Potential causes and risk factors of endometriosis
Altered immunity – Normally, the immune system should be able to eliminate the misplaced endometrium-like cells. Endometriosis patients have less immune cells that clear out these cells 21. However, women with endometriosis are more likely to have autoimmunity, such as Lupus antibodies, thyroid antibodies, and antibodies against the endometrium 222324. They also have higher inflammatory proteins (cytokines), with a tendency towards allergic (Th2) immune response 25. Women with endometriosis are more likely to have allergic conditions, such as allergies, asthma, eczema, and hives as well.
Estrogen dominance or progesterone resistance – Endometriosis lesions outside the uterus depend on estrogen to continue to grow. These lesion cells can also convert testosterone and other forms of estrogen into the most active estrogen (estradiol) 26. Typically, progesterone opposes the growth-stimulating effects of estrogen and helps the endometrium prepare for implantation. However, in endometriosis patients, both the uterine lining and endometriosis lesions may be resistant to progesterone 2728. Because progesterone builds the uterine lining for implantation, the progesterone resistance in endometriosis can contribute to implantation failure 29.
Some modern lifestyle factors can contribute to estrogen dominance, such as toxic ingredients in personal care products and pesticides in conventional meat and produce. Also, not eating enough fiber and constipation may increase estrogen reabsorption 30.
Endocrine disruption – Many environmental toxins act like estrogen (xenoestrogens) or interfere with hormone functions, contributing to the development of endometriosis. Rhesus monkeys develop endometriosis more readily than humans. Exposing these monkeys to dioxins and polychlorinated biphenyls induced the endometriosis 3132. Studies have linked environmental toxins such as toxic metals, dioxins, benzophenones, and phthalates with endometriosis 33. These substances are often found in typical pollution exposures and common household products, such as laundry detergents, cosmetics, soap, and perfumes. However, we need more studies to confirm that these chemicals cause endometriosis in humans. For a great resource on hormone disruptor-free brands, search on the Environmental Working Group’s database.
Environmental Working Group’s Dirty Dozen List of Endocrine Disruptors
| Hormone Disruptor | Most common sources |
| Bisphenol-A (BPA) | Canned food (except BPA-free), cash receipts, polycarbonate plastic |
| Dioxin | Car exhaust and food contamination in meat, fish, and dairy products |
| Atrazine | Corn, water (contaminant) |
| Phthalates | Plastic wraps, PVC, fragrances, scented products |
| Perchlorates | Drinking water, produce, milk |
| Flame retardants | Furnitures, house dusts, carpets |
| Lead | Old paint, and water system in old houses and buildings |
| Arsenic | Rice grown in the US, water (contaminant) |
| Mercury | Larger fish |
| Perfluorinated chemicals (PFC) | Teflon pans |
| Organophosphate pesticides | Non-organic produce and crops that are high in pesticides, such as berries, apples, and leafy greens. Conventional meat, fish, and poultry that are fed with sprayed crops. |
| Glycol ethers | Paint, cleaning products, brake fluids, cosmetics |
Genetics/Family history – Women with first-degree relatives with endometriosis are 5 – 7 times more likely to be diagnosed with it. Also, mothers and sisters of women with endometriosis are much more likely to have endometriosis than those of women without endometriosis. There is no “endometriosis gene,” but genes involved with detoxification, immune function, cell structure, cell overgrowth, and cell migration are linked to endometriosis 3435.
Race – Asian women are most likely to be diagnosed with endometriosis, followed by white, black, and Hispanic women. However, it is unclear whether these diagnosis rates are because the race affects their susceptibility, or if it is due to differences in healthcare seeking and access 36.
Infections – Women with endometriosis are more susceptible to genital tract infections, and the infections may trigger endometriosis. They develop endometrial inflammation due to infections (endometritis) and pelvic inflammatory diseases more readily. These women have less acidic vagina pH, which may allow bad bacteria, such as Gardnerella, Streptococcus, Enterococci, Mycoplasma, and Escherichia coli to grow and affect the endometrium 37. Also, about 11% of endometriosis lesions carry Human Papillomaviruses (HPV) 38. Typically, infections alone do not cause endometriosis, but we need more studies to determine if they are truly a trigger.
How endometriosis affects pregnancy
Endometriosis has been associated with infertility and miscarriage, although some women with endometriosis eventually conceive naturally 39. If you have minimal to mild endometriosis, you may be able to conceive without any medical or surgical intervention. More severe endometriosis, however, makes it harder to get pregnant naturally 40.
Keep in mind, however, that an endometriosis diagnosis is not all bad news. If you’ve had miscarriages and some endometriosis symptoms, it is crucial to get diagnosed and learn how it affects your body. Once you are correctly diagnosed, many treatment options can improve your chances, whether you’re trying naturally or getting fertility treatments (See Endometriosis Treatments).
Endometriosis may increase the risk for the following 4142:
- Infertility
- Miscarriage
- Ectopic pregnancy
- Preterm birth
- Placenta previa
- Small for gestational age infants
- Pre-eclampsia and eclampsia
- Cesarean delivery
Endometriosis and Miscarriage
Endometriosis increases the risk of miscarriage. Interestingly, based on ASRM staging, women with milder endometriosis (stages I and II) are at a higher risk of miscarriage than those with more severe forms (stages III and IV) 43.
However, classifications based on the lesion location alone, i.e., superficial peritoneal, deep infiltrating, and ovarian endometrioma may be more predictive of miscarriage risk. The superficial lesions increase the risk of miscarriage the most, followed by deep infiltrating endometriosis and ovarian endometrioma 4445.
Table: Risk of miscarriage in women with endometriosis, compared to women without endometriosis 46
| Endometriosis classification | Estimated miscarriage risk increase on average (%) |
| ASRM stages I – II | 57% |
| ASRM stages III – IV | 19% |
| Superficial peritoneal | 67% |
| Deep infiltrating endometriosis | 19% |
| Ovarian endometrioma | 11% |
Endometriosis may cause miscarriage by:
Interfering with the implantation process – The endometrium develops each month in response to progesterone, to prepare for implantation and pregnancy. In endometriosis patients, the endometrial tissues are less responsive to progesterone 47. Also, overall high inflammation and free radical production present in this disease disturb the fine balance necessary for implantation and placenta formation 48.
The endometrial tissue may also have an impaired interface with the muscle layer below it (myometrium) inside the uterus, leading to difficult implantation and defective placentation 49.
Reduced egg quality due to the increased inflammation and oxidative stress may increase the risk of miscarriage 50.
Reduced sperm quality – the high oxidative stress and inflammation from endometriosis may reduce sperm quality and cause sperm DNA damage 51.
Impaired embryo transport – the inflammation can reduce the tubal motility and uterine muscle (myometrial) contraction, which can impair the movement of oocytes and embryo to implantation 52.
Structural issues – The scar tissues or adhesions in advanced endometriosis can also trap the ovaries, distort the pelvic anatomy, or restrict the fallopian tubes, contributing to infertility 53.
Diagnosis of Endometriosis
Laparoscopy is the method of choice to diagnose endometriosis. However, your doctor may take several steps to diagnose or rule out endometriosis, including the following steps 54.
Health history
During this medical appointment, you bring up your endometriosis symptoms and history to your OB/GYN. These symptoms may include pelvic pain, painful menstruations (that make you skip school, painful sex, very heavy and prolonged bleeding. Difficulties in passing the stool could also be a symptom of endometriosis. Your doctor may ask clarifying questions about your symptoms, triggers, past treatments, and review your family history and medical history.
Pelvic exam
A pelvic exam can help rule out other conditions that have similar symptoms as endometriosis. This exam only lasts a few minutes. First, your OB/GYN may visually inspect your vagina and vulva. They may also insert a plastic speculum to spread open the vaginal wall. Lastly, they may also manually examine the pelvis with lubricated and gloved fingers.
Ultrasound
An ultrasound exam is a short examination, lasting only a few minutes. It can identify gross abnormalities. It can be done across your belly (transabdominal ultrasound) or through your vagina (transvaginal ultrasound).
Transabdominal ultrasound is performed across the belly. You may be instructed to avoid eating 4-5 hours before the examination and drink a lot of water for better visualization (3-4 glasses of water every half an hour before examination). Your doctor will put the gel on the probe and scan your belly.
Transvaginal ultrasound is performed through your vagina. You should empty your bladder before the examination. Your doctor will put the condom on the probe and the gel over it, and you may feel some discomfort as the probe enters the vagina.
Magnetic resonance imaging (MRI)
An MRI is a radiologic scan used to visualize your organs and tissues with great precision. It might indicate where the endometriosis lesions are spread within the body or how to approach it surgically. The scan is not painful, you don’t need any specific preparation, and it lasts no longer than 15-30 minutes.
Laparoscopy
Currently, laparoscopy (keyhole surgery) is the only way to definitively diagnose endometriosis55. It is a minimally invasive surgery, typically performed under general anesthesia, that allows the doctor to see inside your abdomen.
Your doctor will make a tiny incision near the navel and insert an optic instrument (laparoscope), to visualize the endometrial tissue outside the uterus. Sometimes, they will also take a tissue sample (biopsy) for further analysis.
Although the surgery is minimally invasive, it requires general anesthesia, so you may be advised to avoid eating for at least 6 hours before the procedure 56. The procedure can last from half an hour to around 2 hours.
After the laparoscopy, avoid heavy physical efforts for a week. If you start feeling a fever or abdominal pain, contact your OB/GYN immediately.
Like every procedure with general anesthesia, the risks may include nausea, vomiting, after procedure pain, throat soreness, respiratory failure, cardiac failure, allergic reaction, and death (rarely). Complications are rare but may include bleeding, infection, air embolism, surgical injuries, and pulmonary embolism 57. Also, remember to notify your doctor and share your medical history, especially if you have diabetes or take blood thinners such as aspirin, heparin, or warfarin.
Endometriosis treatments
Pain management
Your doctor may recommend over the counter pain management such as ibuprofen and naproxen sodium to relieve menstrual cramps.
Hormonal therapy
Drug treatment typically does not improve fertility, either during or after treatment. Your doctor may prescribe oral contraceptives, progestins, danazol, and gonadotropin-releasing hormone agonists or antagonists (GnRH analogs). These drugs help with pain or preparation for surgery 58.
Surgical treatment
Currently, surgical removal of endometriosis implants is the only treatment that can improve fertility and relieve pain 59. In most cases, this is done in laparoscopic surgery. However, if the lesions are extensive, your physician may opt for full abdominal surgery instead.
Fertility treatments
Many women with endometriosis may consider fertility treatments to become pregnant. Also, endometriosis may affect up to half of the women seeking fertility treatments 60. Endometriosis decreases the pregnancy rate of in vitro fertilization (IVF), especially in stages III and IV, and those with affected fallopian tubes 61. Endometriosis reduces egg quality, embryo transfer, and implantation rate 62.
However, among women with endometriosis who achieve pregnancy through IVF, the miscarriage rates are comparable to those without endometriosis 636465.
Several studies have confirmed that IVF protocols do not worsen endometriosis 6667. However, it is important to work with a reproductive endocrinologist who is familiar with endometriosis. Because endometriosis is an estrogen-dominant condition, they may use a lower-estrogen protocol. They should also pay attention to your pain, symptoms, and other concerns.
Natural and experimental treatments
Currently, the standard hormonal treatments do not restore fertility, so there is a lot of interest in natural treatments and off-label use of existing drugs. The majority of these studies use pain management as the primary outcome, so we still need more studies to confirm their effects on fertility and miscarriage.
Drugs and natural substances that are being studied for endometriosis may work as 68:
- COX-2 inhibitors. COX-2 is an enzyme that can increase inflammatory fatty acids, such as prostaglandin E2 (PGE2).
- Modulators of estrogen and progesterone function.
- Inhibitors of inflammatory proteins, such as TNF-alpha
- Diabetic drugs that activate PPAR-gamma
- Substances that inhibit the creation of new blood vessels
- Substances that inhibit aromatase enzymes, preventing the conversion of male sex hormones to produce more estrogen
- Stimulating cannabinoid receptors, such as cannabis and cannabis-like drugs 69
- Reducing oxidative stress or inhibiting inflammation by other means
Endometriosis diet
Avoiding red meat – In a study involving 81,908 women and 3800 cases of endometriosis, those consuming more than 2 servings of red meat per day had 56% increased risk of endometriosis. Unprocessed red meat consumption had a stronger effect than processed red meat, but poultry, eggs, fish, and shellfish don’t have the same effects 70. Possibly, red meat may increase inflammation and estrogen in these women 71.
Gluten-free diet – In a study involving 207 women experiencing severe endometriosis symptoms on a gluten-free diet, 75% of them reported a significant reduction in pain. All patients reported improved quality of life 72.
Trans and omega-3 fats – Women who consumed more omega-3 fats were less likely to be diagnosed with endometriosis. In contrast, those who had higher trans fat intake were more likely to be diagnosed with endometriosis 73.
Low FODMAPs diet – FODMAPs stand for Fermentable Oligo-, Di-, Mono-saccharides, And Polyols, which are substances that feed your gut bacteria, such as sugar alcohol, fructose, garlic, and onions. Many people with IBS experience improvement once they avoid FODMAPs. Up to 90% of women diagnosed with endometriosis also have gastrointestinal symptoms, such as bloating, even though bowel lesions were only found in 7.6% 74. In a study involving 160 women with IBS, 36% of them also had endometriosis. Those women with endometriosis were more likely to experience >50% improvement in bowel symptoms 75.
Fruit and vegetable consumption – Fruit intake, especially citrus fruits, is associated with a lower risk of endometriosis. Whereas, the results on vegetable intake has been mixed 76.
Vegetables have a high fiber content that is good for gut health and supports estrogen metabolism which would help lower estrogen dominance.
Ketogenic diets are very low-carbohydrate and moderate protein diets, which force your body to produce ketone for energy. Anecdotally, some women with endometriosis experience significant improvement on ketogenic diets 7778. However, ketogenic diets might not be helpful for all endometriosis patients, and we need more studies to demonstrate its safety and effectiveness.
Dietary Supplements
Supplements denoted with 🅧 are not considered safe for pregnancy.
Omega-3 – Omega-3 reduces COX-2 function 79. In a mouse model of endometriosis, omega-3 supplements inhibit endometriosis cells from implanting 80. A small randomized controlled trial comparing omega-3 and olive oil found some improvement in pelvic pain and well-being in both groups. Possibly, omega-3 wasn’t significantly more beneficial than olive oil because olive oil also contains antiinflammatory substances 81.
Epigallocatechin-3-gallate🅧 (EGCG) is a substance from green tea that inhibits the estrogen-stimulated growth, cell invasion, and blood vessel formation in endometriosis cells 82. However, EGCG is poorly absorbed. There is an ongoing clinical trial to study the effect of EGCG supplement on endometriosis 83 .
Combined supplement protocol – In a small clinical study involving 90 women, combined quercetin, curcumin🅧, parthenium🅧, niacinamide, 5-methyltetrahydrofolate, and omega-3/6 supplements significantly improved endometriosis symptoms, as well as inflammatory blood markers such as PGE2. 84.
Vitamins E and C – 1200 IU of vitamin E and 1000 mg of vitamin C significantly reduced endometriosis-related reduced pelvic pain and inflammation 85.
N-acetylcysteine (NAC) – An Italian study compared 47 NAC-treated and 45-untreated women with endometriomas (endometriosis cysts on the ovaries) for 12 weeks. The treated group received 600 mg of NAC 3 times a day, three consecutive days a week. On average, the treated group had slightly reduced cyst size, with the cysts completely disappearing in 8 women. Whereas, in the untreated group, their cysts grew by 6.6 mm on average and disappeared in 4 of them. 23 NAC-treated patients vs 1 untreated canceled their surgery due to the reduced pain and cyst size by the end of the study period. Overall, 8 women in the treated group and 6 in the untreated group became pregnant 86.
Pycnogenol (pine bark extract)🅧 – 32 women taking 60 mg of pycnogenol were compared with 26 patients taking the drug leuprorelin acetate🅧, a standard treatment, for 48 weeks. Overall, the pycnogenol reduced the pain more slowly than the drug, but there was no rebound effect after the treatments were completed. Among the women taking pycnogenol, 5 of them became pregnant 87.
Traditional Chinese Medicine is a common treatment for endometriosis in China, although most clinical studies only involve small numbers of women 88. One study compared 40 women who took a Chinese herb formula to another 40 who took hormone therapy (mifepristone🅧). The Chinese herb group experienced comparable improvement in inflammatory markers and hormone levels compared to the hormone therapy group. Although not statistically significant, 21 women in the Chinese herb group became pregnant versus 15 in the medication group. However, the miscarriage rate was similar, with 3 miscarriages in the herb group and 2 in the medication group. In the end, 18 out of 40 women in the Chinese medicine group, compared to 13 out of 40 in the medication group, successfully delivered babies 89.
Next Steps to Consider
- If you have been diagnosed with endometriosis, discuss the above treatment options with your doctor
- If you think you might have endometriosis, find a doctor that specializes in working with women with endometriosis who can help with a diagnosis and treatment options
- Stay hopeful! Women diagnosed with endometriosis can go on to have a successful pregnancy.
References

0 Comments