

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- Having the MTHFR gene mutation is common and while it is linked to fertility issues, including miscarriage, the good news is you can address this gene with diet, lifestyle and supplementation
- MTHFR may cause folate deficiency and elevated homocysteine, neither are good for pregnancy.
- Having the MTHFR gene mutation in males is linked to poor sperm health, so it is important to have both partners tested for MTHFR.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Table of Contents
What is MTHFR?
Methylation
MTHFR variants
How MTHFR affects female factors in fertility and pregnancy
How MTHFR affects male factor fertility and miscarriages
Other symptoms of MTHFR variants and poor methylation
What is overmethylation?
Lab Tests for MTHFR and Methylation
MTHFR Treatments
MTHFR and methylation depleters
MTHFR mutations, found in over 40% of the population, may increase the risk of recurrent pregnancy loss 1. It is not only the best-studied but also the most discussed gene in nutrigenomics. However, experts disagree on the real importance of this gene as its effects vary from person to person.
While you can’t change your genes, having the MTHFR mutation isn’t all bad news. There is a lot of research about how you can address it with diet, lifestyle, and supplementation to improve the outcomes. Also, many couples that have MTHFR mutations can have successful pregnancies. In this article, you can read about the health impacts of MTHFR variants and evidence-based ways to address them.
What is MTHFR?
MTHFR stands for methylenetetrahydrofolate reductase, the gene that provides instruction for the production of the MTHFR enzyme. This enzyme is involved in the folate cycle, intersecting with the methionine pathway and the methylation cycle. Because MTHFR is the slowest enzyme in folate activation, it is the bottleneck of the pathway, and thus the most important. Reduced MTHFR function, such as due to MTHFR mutation, can cause both the folate and other pathways to back up, affecting many aspects of health, including fertility.
Is MTHFR mutation bad?
While MTHFR variants may reduce the enzyme function, it doesn’t mean your net MTHFR function is reduced, or that you need to “treat” your MTHFR gene. In fact, most carriers of MTHFR variants have no health problems due to it. The enzyme activity may vary based on cofactors, such as available nutrients, such as riboflavin (see other nutrients for MTHFR).
Your cells can adjust the amount of enzyme produced from the gene with epigenetics. Chemical marks, such as methylation and acetylation, on your chromosomes, can adjust MTHFR gene function. Genetic variants may affect each molecule of MTHFR, but your epigenetics can produce more copies of it. By turning on the epigenetics, you end up with more molecules of the MTHFR enzyme.
Therefore, having an MTHFR variant alone is not all bad news because you can add cofactors and change your epigenetics. In this article, we will cover not only the health risks associated with MTHFR mutations but also how to increase MTHFR activation and production.
Methylation and MTHFR
Methylation is the process of transferring a methyl group, a chemical group with one carbon and three hydrogen from one substance to another. This chemical reaction happens trillions of times per minute in your body.
Methylation helps with hormone production and breakdown, cellular growth and division, DNA and RNA synthesis, amino acid metabolism, and immune balance 3456.
DNA methylation can also turn genes on or off as a type of epigenetic mark, which is important for embryonic development 78. Sensibly, disrupted methylation can contribute to infertility and miscarriages. While methylation on the DNA is a type of epigenetic mark, there are also many other types.
The folate and methionine cycles help produce sources of methyl group (methyl donors) for methylation reactions throughout the body.
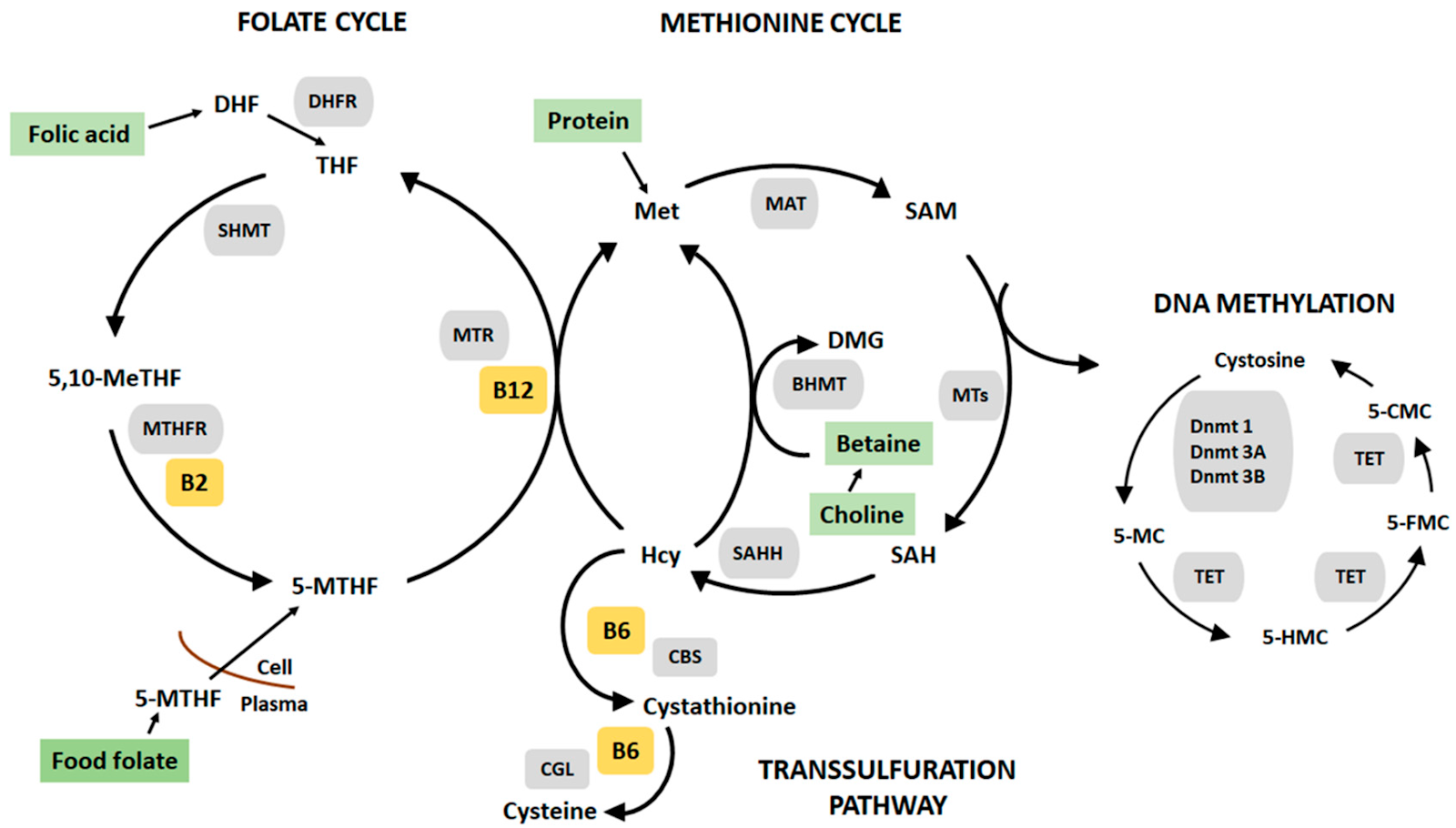
MTHFR is part of the folate cycle, which is linked to the methionine cycle (see image above). In the left-hand cycle, the folate cycle activates folate, generating methylfolate, the form that is readily transported in the blood and used by cells. Whereas the methionine cycle (right-hand side) lowers homocysteine, recycling methionine and generating the methyl donor S-adenosylmethionine (SAM). SAM is then used as a methyl donor for a variety of methylation reactions. Throughout this process, methylfolate, methylcobalamin (methylated vitamin B12), and choline are also methyl donors. These methyl donors are also important for methylation in embryonic development.
Because MTHFR is the most important enzyme in the folate and methionine cycles. Therefore, MTHFR mutation may impact your methylation, DNA synthesis, homocysteine reduction, and ability to use folate. However, other blockages in these pathways, including deficiencies of folate, vitamin B2, vitamin B6, vitamin B12, can have similar effects as MTHFR mutations. Other genes in these pathways may also affect methylation and reproductive health similarly to MTHFR mutation, even in people without MTHFR mutations. This is why studies that associate MTHFR mutations with health issues often provide mixed results.
MTHFR variants
There are hundreds of different MTHFR variants, but the most common ones are C677T and A1298C. Most studies on the effects of this gene relate to C677T.
C677T (rs1801133) changes the default C (cytosine) to T (thymidine). The T in this position reduces the MTHFR enzyme function by about 70%. It substitutes the amino acid at position 222 in the enzyme from alanine to valine 910.
A1298C (rs1801131) changes the default A (adenosine) to C (cytosine). The C in this position substitutes the amino acid 429 of the MTHFR enzyme from glutamine to alanine. Unlike C677T, there is limited research about how this variant affects the MTHFR enzyme activity.
You inherit one copy of the MTHFR gene from each parent. Each of your parents could give you the wildtype (default) version, gene version with C677T, or gene version with A1298C. It is possible but very rare for C677T and A1298C to be in the same copy of the MTHFR gene.
How MTHFR affects female factors fertility and pregnancy
Now that we understand what MTHFR does biochemically, this section will help you understand the effect of low MTHFR and methylation on fertility and pregnancy.
Keep in mind that although folate and methyl donor supplements may help with the following conditions, these supplements alone may not be enough to resolve fertility issues.
Menstrual cycle and ovulation
Methylation is important for tissue growth and cellular development, including the growth of your endometrium and egg during each of your menstrual cycles.
High homocysteine correlates with a lack of ovulation (anovulatory cycles) both in healthy women and those with polycystic ovarian syndrome 1112.
The endometrial growth prepares for the fertilized egg to implant, so disruption in methylation may affect the early stages of pregnancy 1314.
Hormone balance
Homocysteine and healthy folate metabolism are important for hormone balance and hormone responsiveness. Many women with infertility and miscarriage suffer from low luteal phase progesterone.
Some women with higher plasma homocysteine have lower estradiol and lower luteal phase progesterone 15. However, estrogen (estradiol) typically reduces homocysteine, so it’s possible that they have elevated homocysteine because of their low estradiol.
Also, the follicles of women with MTHFR C677T make less estrogen and have ovaries that are less responsive to follicle-stimulating hormone (FSH) during ovulation 1617. Fortunately, higher serum folate is associated with higher luteal phase progesterone, which is healthier for fertility and pregnancy 18.
Methylation is also involved in the breakdown of many hormones, including estrogen, testosterone, thyroid hormone, and progesterone 19. Often elevated homocysteine, which is a sign of poor methylation, will also correlate with hormone imbalances.
Blood vessel health and blood clots
MTHFR and homocysteine may increase the risk of blood clots, especially when other predispositions for blood clot diseases are present 20. Homocysteine is a toxic amino acid that irritates the blood vessels, which can cause problems with the blood vessels. The blood clots and blood vessel problems could interfere with implantation and embryonic development, or cause pre-eclampsia.
Autoimmunity
Homocysteine is an inflammatory amino acid that promotes autoimmunity.
Based on animal studies, elevated homocysteine promotes the inflammatory autoimmune cells called Th17 cells, while folate deficiency reduces the anti-inflammatory cells called regulatory T cells 2122. While homocysteine or folate deficiency alone may not cause autoimmunity, these conditions may precipitate autoimmune disease in the presence of other risk factors. The autoimmune cells may also contribute to miscarriage or other pregnancy complications.
See also our articles on antiphospholipid syndrome and thyroid conditions.
Pregnancy and perinatal issues
MTHFR variants are associated with many pregnancy complications and birth defects. However, most studies in this category show the increase in risk or correlation as it is unethical to do experiments that prove cause and effects in humans. Therefore, MTHFR and folate status are likely one piece of the puzzle rather than the sole cause of these issues.
Implantation failure – Women with C677T and combination of C677T/A1298C are more likely to experience recurrent implantation failure in in vitro fertilization treatments 23.
Pre-eclampsia – Low function of MTHFR gene due to epigenetic and elevated homocysteine are linked to pre-eclampsia 24. C677T, but not A1298C, is associated with pre-eclampsia in Caucasians and Asians 25.
Miscarriage – C677T is linked to an increased risk of early pregnancy loss compared to A1298C and the default MTHFR gene 2627. However, the evidence is mixed on whether MTHFR causes recurrent pregnancy loss 2829.
Intrauterine growth restriction and low birth weight are common pregnancy complications linked to high homocysteine and blood clot disorders. These complications are also linked to MTHFR mutation 30.
Birth defects – C677T and A1298C increase the risk for neural tube defects, cleft lip and palate, and congenital heart disease 313233. However, due to widespread fortification and prenatal supplementation of folic acid, the overall risk of neural tube defects is low regardless of MTHFR variants 3435.
Chromosomal abnormalities – Based on a study of Indian mothers, having two C677T alleles may increase the risk of Down’s syndrome in mothers under 31 years old 36.
How MTHFR affects male factor fertility and miscarriages
Sperm quality and sperm DNA damage
DNA production and DNA methylation are important both for sperm development and viability.
In mice, MTHFR levels are highest in the testis, suggesting that MTHFR is essential for sperm formation. Folic acid supplementation helps improve sperm count and fertility in men who present with infertility 3738. The C677T variant may also contribute to changes in how DNA is packaged into the sperm head 39. However, high dose synthetic folic acid supplementation (5 mg) for extended periods (6 months) may reduce DNA methylation in the sperm by reducing MTHFR function 40.
Also, some men with infertility have reduced MTHFR enzymes in the sperm due to epigenetics 41. Therefore, folic acid supplementation is not beneficial but another downstream metabolite such as betaine may be more helpful for male infertility due to MTHFR 42. However, we only have evidence in male mice, so the clinical evidence behind betaine is lacking.
Other symptoms of MTHFR variants and poor methylation
MTHFR may increase the risk of the following conditions in either gender:
Other diseases of the heart and blood vessel, such as heart disease, pulmonary embolism, and deep vein thrombosis 43
- Mental health issues, such as anxiety, depression, bipolar disorder, and schizophrenia 44
- Chronic fatigue
- Chronic pain
What is overmethylation?
Many people with chronic inflammation have bad reactions when they introduce folate or methylation support supplements. They call these reactions “overmethylation.” However, this is both a misnomer and an oversimplification. Methylation reactions that use SAM participate in numerous cellular processes, including epigenetics, and the production and breakdown of neurotransmitters and hormones.
SAM deficiency, such as due to folate deficiency or MTHFR, may reduce methylation. Correcting SAM deficiency often leads to self-correction from previous undermethylation, especially in growing tissues 45.
However, when there is enough SAM, it is not the sole determinant of these chemical reactions because the human body is not a simple methylation chamber. Numerous other enzymes and proteins that control methylation reactions throughout the body. To classify people as under- or over-methylators based on their health status and reactions to methylation supplements is misleading.
Folate and methylation nutrients, like any other nutrients, affect your epigenetics and turn on or off specific genes. These epigenetic changes are specific to gene, tissue type, and stage of growth rather than an overall increase in methylation 46. Therefore, long-term supplementation with methylation supplements may have unintended health consequences.
Lab Tests for MTHFR and Methylation
MTHFR Genetic Testing
Many medical organizations, such as the American Congress of Obstetricians and Gynecologists and the American College of Medical Genetics recommend against MTHFR genetic testing 47. This is because evidence has been mixed on whether knowing which version of the gene you have is beneficial 48. Some fertility specialists also simply prescribe high-dose folic acid to all their patients (see folate).
However, if you’ve had recurrent miscarriages, it is important to have the full picture. Here are some pros and cons of different test options.
Medical testing for MTHFR in a medically-certified lab is the most reliable, although the most expensive. Your doctor can order these tests and your insurance may cover them. This test is available in all states.
There are also direct-to-consumer testing options such as 23andme or other companies where you receive a large dataset with multiple SNPs. This is the less expensive option that also gives you the data from other genetic variants. However, the result may be less accurate due to the technology that they use. Also, sometimes, your data could be missing certain SNPs, including MTHFR. There may also be privacy concerns with these companies as they sell genetic testing at low costs in order to resell consumer data to drug companies. Some states or jurisdictions, such as New York, New Jersey, Rhode Island, and Massachusetts disallow direct-to-consumer tests.
My Home MTHFR testing is a direct-to-consumer test that only tests one gene, which could be more accurate than whole-genome testing like 23andme.
Blood Tests
Homocysteine
Elevated homocysteine can be a sign of low MTHFR function or folate deficiency. However, kidney disease, thyroid disorders, and vitamin B6 and B12 deficiency can also increase homocysteine. Your homocysteine levels vary with the menstrual cycle and typically go down in pregnancy 495051.
Healthy levels in women 5.8 – 12.8 μmol/L (0.784 – 1.730 mg/L) 52.
Healthy levels of homocysteine in men 53:
- 20 – 39 years old 5.2 – 11.4 μmol/L (0.703 – 1.541 mg/L)
- 40 – 59 years old 5.7 – 12.9 μmol/L (0.771 – 1.744 mg/L)
Fasting total homocysteine (tHCy) normal range is between 5–15 μmol/L (0.676 – 2.028 mg/L).
Elevated homocysteine (hyperhomocysteinemia):
- Moderate 15–30 μM (2.028 – 4.056 mg/L)
- Intermediate 30–100 μM (4.056 – 13.519 mg/L)
- Severe >100 μM (13.519 mg/L)
For pregnancy, the general cutoff is 10 μmol/L.
However, per-trimester reference ranges are also available 54.
- First trimester 3.7–6.9 μmol/L (0.500-0.933 mg/L )
- Second trimester 2.7–7.2 μmol/L (0.365 – 0.973 mg/L)
- Third trimester 2.4–9.6 μmol/L (0.324-1.298 mg/L)
Folate
There are two of folate blood tests—serum or plasma, and red blood cell. Most tests done in the clinic are serum or plasma folate, which measure folate in the liquid part of your blood. Serum folate responds faster to dietary folate, whereas red blood cell folate is more reflective of folate stores and folate turnover in the past 3 – 4 months 55.
The World Health Organization recommends the optimal folate status of >906 nmol/L (or 400 μg/L) red blood cell folate for women of reproductive age to prevent neural tube defects. Other cut-offs in common use are those recommended by the Institute of Medicine are 7 nmol/L for serum/plasma and 305 nmol/L for red blood cell folate to prevent megaloblastic (enlarge red blood cell) anemia in both genders 56.
If you have MTHFR variants or elevated homocysteine, consider checking your folate levels quarterly.
MTHFR Treatments
While we recommend methylfolate as the superior form of folate over folic acid, many physicians recommend folic acid. Here we are presenting the evidence regarding both forms of folate, along with the pros and cons.
Folic Acid
The general medical recommendation is to ensure that you consume at least 400 – 600 micrograms (µg) of dietary folate daily. Your doctors may advise you to supplement with 600 micrograms of folic acid daily as a prenatal supplement. Folic acid is also a typical part of prenatal multivitamins.
If you have had multiple miscarriages or fertility issues, your doctor may prescribe a pharmaceutical dose of 4 – 5 milligrams (= 4000 – 5000 micrograms). However, there is no evidence to support the use of 5 milligrams folic acid from preconception to reduce the risk of miscarriage 57. Also, folic acid supplementation may not help with miscarriages 58.
Is folic acid bad for MTHFR?
Differences between folic acid and folate – Folate is the collective term that refers to all types of vitamin B9, including folic acid, methyl folate, and other folate metabolites. Folic acid is the synthetic form of folate that is more shelf-stable and more readily absorbed.
Because folic acid has been fortified and prescribed for decades, we have a lot of clinical and epidemiologic evidence supporting its safety and effectiveness. Folic acid has effectively reduced neural tube defects and low birth weight in populations that include all forms of MTHFR 5960. Therefore, most medical doctors are more comfortable with folic acid than methylfolate. However, the lack of long-term or large studies on other forms of folate does not mean that they are not safe or effective.
When you have MTHFR, methylfolate seems like the most logical option because it is the active form of folate and the product that the MTHFR enzyme creates. Methylfolate bypasses MTHFR and other enzymes to activate it.
Cancer risk – More recent molecular evidence suggest folic acid may not be the best treatment, especially at high doses. Folic acid requires the conversion of another enzyme dihydrofolate reductase (DHFR), which is a very slow enzyme. Very high doses of folic acid can overwhelm DHFR and result in unmetabolized folic acid in the blood, which may contribute to cancer 6162. On the other hand, methylfolate is the form of folate that naturally circulates in the blood, so it is less likely to introduce a health risk.
Too much folic acid can also induce a folate deficiency. There is a case study of a 41-year-old woman without MTHFR mutation using 5 milligrams of folic acid daily for fertility treatment. After 4 months of high-dose folic acid, she developed high homocysteine. Once she switched over to 500 micrograms of methylfolate, her homocysteine levels drop. The fertility clinic that treats this patient also reported their anecdotal findings that many of their patients with MTHFR mutations have better results with methylfolate, with homocysteine levels dropping within 10 days 63. Nowadays, many fertility specialists are also recommending methylfolate in their practice.
High folic acid changes epigenetics – In a study with 30 men with infertility of unknown causes, 5 milligrams folic acid supplementation increased blood folic acid but not sperm parameters after 6 months. Overall DNA methylation throughout the genome decreased more in C677T carriers than others 64. Therefore, very high doses of folic acid for long periods of time may be harmful, but we need larger studies to confirm the effects.
Recommendation: 400 micrograms of total dietary folate for general health or 600 micrograms for prenatal. With MTHFR variants, methylfolate may be more beneficial at around 500 micrograms. Long-term supplementation of high-dose folic acid is not recommended.
Other nutrients for MTHFR
Folate works with other B vitamins in the folate and methionine cycles. Therefore, natural folate found in foods typically is present with these other B vitamins. Therefore, if you supplement with folate, it is important to also supplement these other vitamins. These supplements, except for creatine, are safe for pregnancy at doses indicated below, although it may be better to obtain these nutrients from foods.
Riboflavin (vitamin B2) is a part of a cofactor of MTHFR. Many people with C677T have high homocysteine because they are deficient in riboflavin. Riboflavin supplementation in C677T carriers reduce homocysteine 6566. The daily recommended intake is 1.4 mg during pregnancy and 1.6 mg during lactation. Upper limit (toxic levels) for riboflavin intake has not been reported 67.
Methylcobalamin (methylated vitamin B12) is an important cofactor for another key enzyme in the folate pathway, methionine synthase (MTR). Methylcobalamin is also a methyl donor, but cyanocobalamin, a common supplemental form of vitamin B12, is not 68. Doses of up to 50 micrograms have been safely used in clinical trials in pregnant women. The clinical trials showed that the B12 supplement reduced pregnancy complications 69.
Choline and betaine are methyl donors that are not dependent on the folate pathway. It may provide compensation for lowered function of MTHFR. When men with C677T take high-dose choline (2200 mg), they have increased cellular methylation but reduced DNA damage, but also have increased homocysteine level 70. Choline is safe for up to 3.5 grams/day in adults, and 550 – 900 mg/day during pregnancy 71.
Creatine🅧 – The methylation of guanidinoacetate to form creatine consumes more methyl groups than all other methylations in the body combined 72. Therefore, creatine supplementation may reduce the need for methylation resources. In a case study, 5 grams/day of creatine supplementation in C677T carrier reduced homocysteine 73. 5 grams is a typically safe dose for adults. While creatinine may be beneficial during pregnancy, there is no evidence about its safety during pregnancy, so it is not recommended for pregnancy 74.
Pyridoxal-5-phosphate or pyridoxine (vitamin B6) is an important cofactor for the cystathionine-beta-synthase enzyme, which breaks down homocysteine independent of MTHFR 75. Vitamin B6 is safe to take during pregnancy and may help with morning sickness. Doses of 510 mg have been safely used in clinical trials to treat morning sickness in pregnant women, although 3 mg should be sufficient for nutrition status 7677.
Zinc deficiency impacts methylation, methionine metabolism, and protein synthesis in animal models 78. Also, zinc supplementation of between 5 – 50 mg may help with many common pregnancy and birth complications 79.
Diet and lifestyle changes for MTHFR
There is no diet that can treat an MTHFR gene. Generally, you should focus on a balanced diet rich in whole food sources of folate, such as leafy green vegetables, legumes, meat, and nut butters. Liver also contains a lot of folate, although the high vitamin A levels in the liver may not be safe for pregnancy. Fortified (enriched) foods, such as pasta, cereal, and flours are also good sources of folic acid.
Also, manage stress. Mental-emotional stress places a demand on your methylation pathways and may increase homocysteine 80.
MTHFR and methylation depleters
The following factors deplete the methylation pathway. However, if your physician prescribes these medications, you should not avoid the medications just because they deplete the methylation pathway. In some cases, you need to take the medications without the folate for it to work. In other cases, your doctor may recommend that you supplement with folate and/or other methylation nutrients along with these medications. Therefore, you should always discuss your supplementation with your doctor and pharmacist because of these supplement-drug interactions.
Medications
These medications, except for stomach acid-lowering drugs, are generally not safe and not recommended for pregnancy. However, we are aware that many women with miscarriages may be prescribed these medications at some point.
- Methotrexate depletes folate, but supplementing with folate could make the medication less effective 81. Methotrexate is a treatment for ectopic pregnancy, cancer, and some autoimmune conditions. You may want to discuss with your doctor about taking folate once your treatment is complete.
- Hormonal birth control pills
- Metformin is a treatment for polycystic ovarian syndrome and diabetes
- Stomach acid-lowering drugs
Supplements
- Vitamin B3 (Niacin) and its derivatives, including niacinamide, nicotinamide adenine dinucleotide, nicotinamide riboside, and nicotinamide mononucleotide
Lifestyle
- Alcohol
- Smoking
Note: This article may contain affiliate links. We appreciate your support of Miscarriage Hope Desk!
Next Steps to Consider
- Look into getting tested for the MTHFR mutation for both you and your partner. Click here for a resource that offers testing.
- If you do have the MTHFR mutation, work with your doctor or other health care professional to incorporate the supplementation and lifestyle suggestions outlined, above
References

I have just discovered this website and it’s brilliant. I have had 3 miscarriages (one of which was twins, so it definitely feels like 4 to me!), followed by a rather traumatic breakdown of my relationship with my ex so I am now embarking on IVF with donor sperm. I am desperate to try and resolve the RM issue and like you, have read loads about infertility and often feel RM is overlooked. Commonly, the implication is that getting pregnant is the goal rather than having a baby. My RM tests show that I am heterozygous for the C677T mutation of MTHFR so your article here has been so helpful. It is clear, concise, evidence-based and objective and it gives me hope. Thank you.