

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are the key takeaways I would share with you as a friend:
- Elevated homocysteine can contribute to infertility and miscarriage. This article takes an in-depth look at how.
- Homocysteine is not routinely tested, but should be considered for both the female and her male partner.
- Luckily, there are ways to treat elevated homocysteine and this article takes an in-depth look at best treatment options, which depend largely on the root cause of the elevated homocysteine.
I also recommend you do your own research and work with your doctor. That is why I have coordinated these articles with the nitty-gritty details and links to research so you can make an informed decision on what works best for you… read on for more! And don’t miss my Next Steps section at the bottom.
Table of Contents
What is homocysteine?
Health effects of homocysteine
How is homocysteine created
Disorders of Elevated Homocysteine
Causes and risk factors for hyperhomocysteinemia
Diagnosis of hyperhomocysteinemia
Treatment for hyperhomocysteinemia
Elevated homocysteine levels are associated with folate deficiency and infertility. However, there is mixed evidence on whether it causes miscarriage 1.
Due to the mixed evidence, homocysteine is often overlooked as part of a miscarriage workup. Also, it can aggravate polycystic ovarian syndrome and blood-clotting disorders, and increase the risk of pregnancy complications2. Therefore, if your homocysteine is high, it is important to address it for a healthy pregnancy.
Importantly, folate deficiency is not the only reason homocysteine could be high, and sometimes only taking high-dose folic acid could make hyperhomocysteinemia worse.
This article summarizes the latest research about high homocysteine, how it affects your health, pregnancy and miscarriage risks, and what you can do about it.
What is homocysteine?
Homocysteine is a sulfur-containing amino acid naturally produced in our bodies as a metabolite of essential amino acid methionine3.
It is an inflammatory and toxic amino acid that can damage the blood vessel, contributing to blood clots and cardiovascular diseases4.
Because healthy blood vessels and folate levels are important for a pregnancy, high homocysteine can make it difficult to conceive and maintain a pregnancy.
Health effects of homocysteine
Homocysteine can affect health and fertility via the following activities 5.
Homocysteinylation – homocysteine can attach itself to proteins and tissues, impairing their function or resulting in an autoimmune response. This may lead to blood clotting.
Inflammation – homocysteine promotes inflammation throughout the body. It can contribute to inflammatory conditions and infertility.
Increasing oxidative stress – homocysteine promotes oxidative stress and inhibits antioxidant enzymes in the body. The pro-oxidative activity can be harmful for eggs, sperms, and embryos.
Neurotoxins – High levels of homocysteine can be neurotoxic, contributing to neurologic and mental health disorders.
Symptoms and health effects of elevated homocysteine
Many people with elevated homocysteine have no symptoms until it manifests as blood clots or cardiovascular conditions.
Some people with severe B vitamin deficiencies that lead to high homocysteine may also experience symptoms of these deficiencies, such as anemia symptoms.
Because homocysteine is neurotoxic, some people with elevated homocysteine may experience cognitive dysfunction and increased risk of dementia 6. Some studies have also associated homocysteine with mental health disorders such as anxiety and depression 7.
Hyperhomocysteinemia is often found in and exacerbates kidney disease, bone tissue damage, digestive disorders, and cancers 8.
Effects of homocysteine on female fertility and hormones
Estrogen tends to lower homocysteine. Because methylation is important in hormone production and breakdown, homocysteine often correlates with hormone imbalances or lower fertility.
High homocysteine correlates with lack of ovulation (anovulatory cycle) both in healthy women and those with polycystic ovarian syndrome 910.
Also, women with higher homocysteine due to lower estrogen tend to have lower luteal phase progesterone and higher follicle stimulating hormone at ovulation 11. Also, the blood vessel-damaging effects of homocysteine could damage the endometrium and disrupt the implantation, which can lead to a chemical pregnancy 12.
Many women with unexplained fertility have elevated serum homocysteine 13. Treatments that lower homocysteine improve their fertility outcomes 14. Among infertile women receiving fertility treatments, lower homocysteine in the follicular fluid was associated with better chance of clinical pregnancy 15.
Polycystic ovary syndrome (PCOS) patients with elevated homocysteine are significantly more likely to suffer from repeat miscarriage than those with normal homocysteine levels 16. In some cases, treatments with diabetic drugs, such as metformin and rosiglitazone, may increase homocysteine 17. Given that PCOS increases cardiovascular risk, high homocysteine should be tested and treated.
Effects of homocysteine on male fertility and hormones
Folate is important for DNA synthesis and re-methylation of homocysteine into methionine. High homocysteine, a typical sign of low folate, may impair sperm production due to reduced DNA synthesis and abnormal methylation 18.
The inflammation from hyperhomocysteinemia can lead to impaired sperm parameters and infertility. The increased oxidative stress can damage sperm DNA. Also, homocysteine impairs healthy circulation, which is important for male sexual function. Homocysteine also reduces nitric oxide production, which is important both for male sexual function, sperm production, and fertilization process .192021 Among couples undergoing IVF, higher homocysteine leads to lower quality embryos22.
Homocysteine in pregnancy and miscarriage
During pregnancy, homocysteine levels decline to the lowest during the second trimester, and increase again in the third trimester 23. This fluctuation happens due to 24:
- Increase in kidney filtration rates during pregnancy
- Blood volume expansion during pregnancy25
- Increased homocysteine uptake by the fetus
Neural tube defects and cleft palate are the most recognized birth defects associated with folate deficiency and high homocysteine. However, elevated plasma homocysteine is also associated with many pregnancy complications, including 26:
- High blood pressure complications, such as preeclampsia and placental abruption
- Recurrent early pregnancy loss due to blood clots or blood vessel damage
Homocysteine may aggravate the following pre-existing blood clotting disorders and further increase the risk of miscarriages.
How is homocysteine created 3132
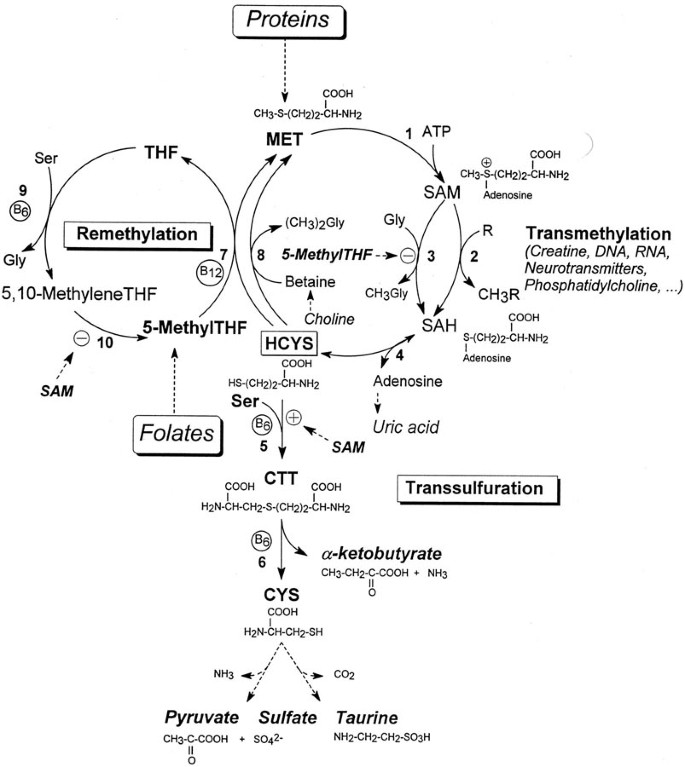
Homocysteine and methionine are part of one-carbon metabolism or methylation pathway.
Once a methionine donates a methyl group, it becomes homocysteine. There are many ways to convert homocysteine into a less toxic substance. It can receive the methyl group again to become methionine, or broken down into the amino acid cysteine via the transsulfuration pathway.
In re-methylation, the enzyme methionine synthase takes the methyl group from methylfolate (MTHF) and gives it to homocysteine, using vitamin B12 as a cofactor.
Homocysteine can also receive the methyl group from betaine or trimethylglycine, catalyzed by the enzyme betaine-homocysteine methyltransferase (BHMT).
During transsulfuration, the enzyme cystathionine-β-synthase (CBS) converts homocysteine into cysteine using vitamin B6 as a cofactor.
Any compromise in these processes or enzymes can increase homocysteine levels.
Disorders of Elevated Homocysteine
There are two distinct disorders that can both result in elevated homocysteine.
Homocystinuria is a rare congenital disorder most commonly caused by severe mutations, such as isoleucine to threonine at position 278 and glycine to serine at position 307 in the CBS gene 34. However, severe mutations in other genes involved in homocysteine metabolism, such as MTHFR, MTR, MTRR, and MMADHC can also homocystinuria. The severe mutations are typically recessive, meaning you need one mutated copy from each of your parents, so homocystinuria is very rare.
This disorder increases homocysteine and related metabolites. Symptoms include nearsightedness, osteoporosis, neurologic and skeletal developmental problems, and blood clotting 35. People with homocystinuria typically have extremely high homocysteine of >100 µmol/L and methionine >50 µmol/L, when normal ranges are <15 µmol/L and 10 – 40 µmol/L, respectively 36.
Hyperhomocysteinemia, a more common disorder, refers to slightly elevated homocysteine of over 15 µmol/L due to other causes than severe genetic mutations. Approximately 5 – 7% of the population have mild hyperhomocysteinemia 37.
Causes and risk factors for hyperhomocysteinemia
1) MTHFR variants
The C677T and A1298C variants of MTHFR are present in 20 – 40% and 7 – 12% of the population, respectively. C677T results in MTHFR enzymes with 70% reduced function, whereas A1298C results in MTHFR enzymes with 40% reduction of function. Nevertheless, these are considered mild mutations because they don’t singlehandedly cause congenital birth defects, unlike more severe mutations. However, folate deficiency together with C677T and A1298C variants may increase some health risks 38.
Both variants of MTHFR increase the risk of hyperhomocysteinemia 3940.
2) Variants affecting other genes in the folate pathway
MTHFR is not the only gene that confers risk of elevated homocysteine. Many other common variants in enzymes in the folate pathway may also increase the risk of hyperhomocysteinemia, such as 4142:
- A 19-base pair deletion within the Dihydrofolate reductase (DHFR) gene
- Not having the 68-base pair insertion within the CBS gene
- The deletion of the Thymidylate Synthase (TYMS) gene
- The A allele at position 2756 of the Methionine Synthase (MS) gene
Having multiple of these variants may result in higher homocysteine than one of them 43. Because these variants affect the production of methylfolate, ensuring sufficient folate and other cofactors is likely to overcome the associated risks. Also, testing the phenotype, such as blood tests for homocysteine, is more clinically useful than testing these genes.
3) Deficiency of vitamin cofactors
Insufficient amounts of cofactors involved in the metabolism of homocysteine, such as vitamins B2, B6, B9, and B12, increase the risk of hyperhomocysteinemia 44.
4) Kidney problems
The kidneys remove about 15% of plasma homocysteine and are responsible for removing any excess homocysteine. Therefore, any factors that affect kidney function can increase homocysteine 45. About 85% of chronic kidney disease patients have hyperhomocysteinemia 46. The elevated homocysteine also tends to further damage the blood vessels and impair kidney functions.
5) Hypothyroidism
The thyroid hormones may influence the activities of enzymes that break down homocysteine in the liver and the kidney filtration rates 4748. Therefore, low or suboptimal thyroid function can lead to hyperhomocysteinemia 4950.
6) Medication
Many medications may increase homocysteine levels. Cholestyramine and metformin interfere with folate absorption in the gut. Whereas, methotrexate, nicotinic acid (niacin), fibric acid derivatives, diabetic drugs, and oral contraceptive pills may interfere with folate or homocysteine metabolism 51.
7) Digestive problems
Digestive problems such as celiac disease and inflammatory bowel disease may reduce vitamin absorption and contribute to elevated homocysteine 52.
8) High-protein diets
High-protein diets, especially ones high in muscle meats, can temporarily increase homocysteine levels 24 hours after meals. However, dietary intake alone doesn’t increase fasting homocysteine in healthy people 53.
Diagnosis of hyperhomocysteinemia
Currently, there is limited clinical evidence that confirms that homocysteine causes miscarriage, although it is highly plausible. Therefore, major reproductive medicine organizations do not recommend homocysteine or MTHFR testing for recurrent pregnancy loss 54. These include the American Society of Reproductive Medicine and the European Society of Human Reproduction and Embryology,
Some research groups believe that in young people with advanced cardiovascular disease, homocysteine levels should be measured 55. Although miscarriage doesn’t fit into this category, blood vessel damage in the placenta could be an indication for homocysteine testing.
Plasma homocysteine is about 70% bound to albumin, and the remaining 30% forms low molecular weight disulfides, predominantly with cysteine. The sum of all these Hcy species is termed total Hcy, abbreviated tHcy 56.
Although homocysteine varies during the menstrual cycle and pregnancy, there is no consensus of when during menstrual cycle or pregnancy the homocysteine levels should be tested.
Homocysteine blood test reference values in μM and mg/L
Healthy levels in women 5.8 – 12.8 μM (0.784 – 1.730 mg/L)57.
Healthy levels of homocysteine in men 58:
- 20 – 39 years old 5.2 – 11.4 μmol/L (0.703 – 1.541 mg/L)
- 40 – 59 years old 5.7 – 12.9 μmol/L (0.771 – 1.744 mg/L)
Fasting total homocysteine (tHCy) normal range is between 5–15 μM (0.676 – 2.028 mg/L).
Elevated homocysteine (hyperhomocysteinemia):
- Moderate 15–30 μM (2.028 – 4.056 mg/L)
- Intermediate 30–100 μM (4.056 – 13.519 mg/L)
- Severe >100 μM (13.519 mg/L)
For pregnancy, the general cutoff is 10 µM (1.352 mg/L). However, per-semester reference ranges are also available 59.
- First trimester 3.7–6.9 µM (0.500-0.933 mg/L )
- Second trimester 2.7–7.2 µM (0.365 – 0.973 mg/L)
- Third trimester 2.4–9.6 µM (0.324-1.298 mg/L)
Methionine loading test
The methionine loading test is a controversial test to assess hyperhomocysteinemia. Some people with reduced ability to detoxify homocysteine have normal fasting homocysteine level but highly elevated homocysteine after consuming methionine. For this test, you consume 0.1 g per mg of bodyweight of methionine during fasting, and get a blood draw for a homocysteine test 6 hours later 60.
This test may also specifically indicate low function of the CBS enzyme 61.
Treatment for hyperhomocysteinemia
If you experienced pregnancy loss or difficulties in conceiving and have hyperhomocysteinemia, the good news is that elevated homocysteine can be easily treated.
Most cases of hyperhomocysteinemia are treatable with nutrition, but it is also important to address other contributing factors. In some cases, if homocysteine does not normalize with increasing supplementation, it is likely other issues (see causes and risk factors above) than the vitamin deficiency that contributes to it 62.
B vitamins and cofactors
Vitamins that take part in homocysteine metabolism are necessary for multiple reasons, and they daily requirements are following 6364:
| Vitamin | Preconception | Pregnant | Lactating |
| B2 | 1.4 mg | 1.4 mg | 1.6 mg |
| B6 | 1.3 mg | 1.9 mg | 2.0 mg |
| B12 | 2.4 μg | 2.6 μg | 2.8 μg |
| Folate | 400 μg | 400-600 μg | 600 μg |
Some doctors may prescribe a pharmaceutical dose of folic acid at 4000 – 5000 μg (4 – 5 mg) for couples who struggle to conceive. If you take this dose, it is important to re-check your homocysteine level. Folic acid requires the DHFR enzyme, which is a slow enzyme, to convert into a usable form. Very high dose of folic acid can overwhelm DHFR 65. Also, excessive unmetabolized folic acid may compete with more biologically active folate, causing a folate deficiency state. In a case study, a 41 year old woman with normal MTHFR developed hyperhomocysteinemia with 5 mg of folic acid during her fertility treatment. Her homocysteine normalized once she switched to 500 μg of methyl folate 66.
Improved diet and lifestyle
Interestingly, treatment of high homocysteine with folic acid successfully reduces homocysteine but does not reduce the risk of cardiovascular diseases 67. This is possibly because cardiovascular conditions are lifestyle-related conditions that require more than folic acid to address. However, healthy diet, lifestyle, stress management and sleep are essential both to lower cardiovascular risk and improve fertility.
For more info on folic acid vs methyl folate, check out our MTHFR article.
Anti-clotting therapy
Some patients may be prescribed medications that reduce blood clots if they have MTHFR or elevated homocysteine. Although the American Society of Reproductive Medicine does not recommend this, some OB/GYN may prescribe it with empirical value.
If you have elevated homocysteine and repeat miscarriage, speak to your doctor about ruling out other blood clotting disorders, such as antiphospholipid syndrome, and conditions such as PCOS.
Conclusion
Although the science is clear that high homocysteine is unhealthy and may increase blood clots, it is not often tested in a miscarriage workup.
MTHFR is not the only cause of elevated homocysteine. Other factors that increase homocysteine, such as kidney and thyroid issues should be also addressed. Also, folate supplementation alone might not normalize homocysteine if these other causes are at play. Therefore, it is important to test before and after the treatment with folate.
Next Steps to Consider
- Request your doctor test both you and your partners homocysteine levels.
- If you do have elevated homocysteine, it is important to work with a doctor or other health care professional to understand what might be causing these elevated levels.
- The good news is that once you recognize, understand and treat elevated homocysteine levels, you will improve your chances of a healthy pregnancy.
References

0 Comments