

Hi, my name is Allison Schaaf, my own fertility journey, including 5 miscarriages, inspired me to create this website to help YOU navigate your own fertility journey.
Here are my main takeaways I would share with you as a friend:
- PCOS is the most common cause of infertility and increases the risk of miscarriage.
- This article discusses research related to PCOS and fertility and also touches on changes you can make to diet, lifestyle and other steps to improve fertility.
- Women with PCOS can have this condition under control and maintain healthy pregnancies.
Of course, I also recommend you do your own research! That is why I have coordinated these articles with the nitty-gritty details and links to research so you can best decide what works best for you, read on for more! And don’t miss my Action Steps at the bottom of the article!
Table of Contents
What is PCOS?
Risk factors and triggers for PCOS
PCOS Symptoms
How PCOS affects pregnancy, fertility, and miscarriage
Pregnancy complications of PCOS
How PCOS is diagnosed
Treatment for PCOS
Polycystic ovary syndrome (PCOS) affects about one in 15 women worldwide 1. In the USA, it is the most common cause of infertility 2. PCOS increases the risk of pregnancy complications, including miscarriages 34.
As a complex and somewhat controversial syndrome, PCOS is often misdiagnosed. In a large study involving over 1385 women, one-third of them took over two years to get diagnosed. Also, nearly half (47%) saw three or more health professionals before finally getting diagnosed with PCOS 5. The diagnosis process, along with the unmet medical and emotional needs, can be very stressful.
Fortunately, you can manage many aspects of PCOS with diet and lifestyle, and many women with PCOS have had successful pregnancies 6. This article will provide you with everything you need to know about PCOS and recurrent pregnancy loss (RPL).
What is PCOS?
Polycystic ovarian syndrome is a hormonal and metabolic disorder that disrupts ovarian function. It may prevent normal development of the uterine lining and the egg, or cause cysts in the ovary.
It is a syndrome rather than a disease because it has more than one clinical feature or symptoms. None of the PCOS symptoms or blood markers are reliably present in all PCOS patients. Therefore, doctors diagnose it mainly based on clinical presentation rather than a specific laboratory or imaging criteria.
Risk factors and triggers for PCOS
PCOS is a multifactorial condition with multiple contributing causes, which may include:
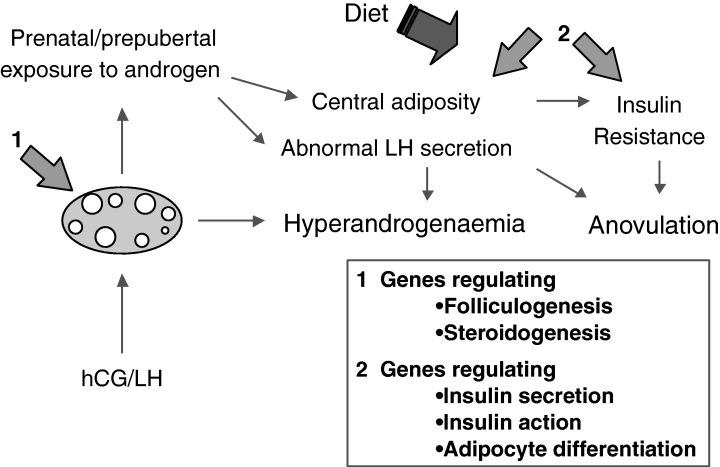
- Metabolic disturbances during pregnancy of the patient’s mother, such as gestational diabetes, elevated testosterone or elevated Anti-Müllerian Hormone (AMH) 7
- Genetics – genes involved in steroid hormone production and metabolism, Luteinizing Hormone (LH) and its receptors, insulin and diabetes-related genes, genes related to inflammation, and PAI-1 8
- Obesity and weight gain
- Type 1, type 2 and gestational diabetes, and metabolic syndrome 9
- Autoimmunity in some women with PCOS 10
- Infections and environmental toxins (speculative) 11
PCOS Symptoms

The latest research found that PCOS may start in utero in predisposed females. Then, the symptoms start to show during puberty and get worse as they 13. Menstrual irregularities usually start with first menstruation (menarche) along with male pattern hair growth 14.
PCOS symptoms may include 1516:
- mild obesity or weight gain
- irregular (>35 days for >6 months, or <9 periods/year) or lack of menstrual cycles for >6 months, caused by hormone imbalances leading to irregular ovulation 1718
- male sexual characteristics due to excess male sex hormones, such as excess hair growth (hirsutism), balding, and acne
- Infertility, defined as the inability to conceive for over 1 year of unprotected sex
- Acanthosis nigricans (thickened and darkened skin in the armpit, on the nape of the neck, in skin folds, and on knuckles and/or elbows) due to insulin resistance 19
- Mental health problems such as anxiety, depression, and headaches due to neurological and hormonal imbalances 20. Infertility and miscarriages may also worsen these mental health problems.
Aside from the symptoms above, the hormonal hallmarks of PCOS include:
Excess male sex hormones, such as testosterone and DHEA, can cause secondary male characteristics such as facial, back, and chest hair accompanied by body odor. Typically, the hair is present around the nipple and following down the midline (linea alba) of the abdomen to the pubis, along with temporal hair thinning 21. PCOS acne tends to be along the jaws 22.
High insulin (hyperinsulinemia) and insulin resistance are hallmarks of PCOS. Insulin resistance may not always cause obesity, but obesity always exacerbates it 23. Obesity itself may contribute to infertility and the risk of pregnancy complications. About 50% of women with PCOS are overweight or obese, whereas the other 50% are normal weight or even underweight 24.
How PCOS affects pregnancy, fertility, and miscarriage
In PCOS, hormonal disruptions can throw off the following processes that are essential for conception and healthy full-term pregnancy.
Oocyte development and ovulation
During a normal cycle, the hormones, Follicle Stimulating Hormone (FSH) and LH, work together to nurture and grow a follicle (egg sacs of immature eggs), which later releases an oocyte. LH acts on theca cells in the ovary to produce androgens (male sex hormones). Then, FSH acts on granulosa cells to induce androgen conversion to estrogen. An estrogen surge leads to the LH surge, which induces ovulation 26.
In PCOS patients, disturbed LH and FSH secretion prevent normal development of the oocytes and ovulation, which can lead to a lack of ovulation and menstruation 2728. When the oocytes are not released, the follicles keep developing and become cysts in some women. Even when there is ovulation or an IVF treatment, the oocyte may not be competent enough to fertilize and develop into a healthy fetus 29.
FSH and LH are often both in the range of about 5-20 mlU/ml in young fertile women. In women with polycystic ovaries, LH is typically two to three times that of FSH, which may disrupt ovulation 30.
Sex hormone imbalances
In PCOS, sex hormone-binding globulin (SHBG) decreases, which increases free testosterone 31. The ovaries also produce excess male sex hormones due to the combination of insulin resistance and LH stimulation. Estrogen levels tend to be normal because some of the male sex hormones could be converted into estrogen.
During pregnancy, the elevated androgens and increased androgen receptors in the endometrial cells may also interfere with embryoic implantation and development 3233.
Normally, progesterone feeds back to the hypothalamus to help stop excess LH production, but the hypothalamus of women with PCOS is resistant to progesterone 34. Progesterone is an important hormone that helps to initiate and maintain pregnancy. In women with PCOS, the endometrium is also less responsive to progesterone 35. This may explain why progesterone therapy or birth controls that contain progesterone may be helpful (see Medications).
Uterine and endometrial development
Typically, after ovulation, the follicle that released the egg becomes the corpus luteum and produces progesterone in order to prepare the uterine lining for the embryo. If pregnancy does not occur progesterone levels drop, resulting in menstruation.
With PCOS, it is common for women not to ovulate. Also, without menstruation, the uterine lining does not shed and renew each month, leading to a thicker lining that is less prepared for embryo implantation 36. The thicker lining can prevent a successful embryo implantation in the first few days of pregnancy, which can lead to early pregnancy failure 37. With the extra uterine lining build-up, some PCOS women also experience excessive bleeding once they menstruate 38.
Increased Plasminogen Activator Inhibitor-1 (PAI-1) Levels
Plasminogen activator inhibitor-1 (PAI-1) is a protein that causes blood clots, which can cause miscarriage and pregnancy complications 39. Many women with PCOS have high PAI-1. For some, metformin and ovarian drilling (a keyhole surgery to stimulate ovulation) reduced PAI-1, while for others PAI-1 remains high because PCOS is different for everyone. Among those who received these treatments, the reduction of PAI-1 correlated with better pregnancy outcomes 40.
Whereas, metformin-treated women who still had high PAI-1 were still more likely to have early miscarriage 41. Therefore, based on small studies thus far, reducing PAI-1 may be a determinant of successful pregnancy in PCOS. If you suffer from PCOS and recurrent miscarriage, consider asking your doctor about the PAI-1 test.
Elevated Anti-Müllerian hormone
Anti-Müllerian hormone (AMH) is released from developing follicles. It is a measure of ovarian reserve, or the quality and quantity of eggs you have left in store. The best range of AMH for pregnancy is 1 – 4 ng/mL 42. Without PCOS, higher AMH is better for conception. Very low AMH of 0.7 ng/mL in older women often predicts difficulty to conceive due to age-related egg depletion 4344. Whereas, levels less than 0.4 ng/mL may predict an increased risk of miscarriage 45.
Women with PCOS have elevated AMH of >4.9 ng/mL due to the accumulation of follicles in their ovaries 46. The high AMH may be a diagnostic marker for PCOS 47.
In addition, pregnant women with PCOS have elevated AMH during pregnancy 48. High pregnancy AMH is associated with preterm delivery and may contribute to the development of PCOS in the child 4950. The abnormally elevated AMH in PCOS often normalizes with effective PCOS treatments. For example, small clinical studies showed that exercise and metformin reduced AMH 5152.
Elevated homocysteine
Hyperhomocysteinemia is linked to recurrent pregnancy loss and many other pregnancy complications, possibly because it reflects folate and/or B vitamin deficiency. In addition, elevated homocysteine may cause type 2 diabetes 53. However, many PCOS patients also have high homocysteine regardless of insulin resistance, disease severity, and metformin treatment 54. Possibly, genetic or lifestyle factors that elevate homocysteine, such as C677T MTHFR variants and folate deficiency, may worsen PCOS. (Read our article on MTHFR, linked here).
Pregnancy complications of PCOS:
Miscarriage
Although PCOS disrupts many important processes for a healthy pregnancy, it remains controversial whether PCOS causes miscarriage. A meta-analysis (combined analyses of small clinical studies) found that PCOS is linked to nearly 3 times the risk of miscarriage, whereas another found no association 5556. Among these, miscarriages in PCOS tend to happen in the first trimester 57. However, how PCOS affects pregnancy can vary greatly from case to case. Some women with PCOS have successful pregnancies, while others present with miscarriages or other complications.
With in vitro fertilization (IVF) pregnancies, PCOS women are at ~41% increased risk of miscarriage than those without PCOS 58. Treatment with ovulation-inducing agents is also associated with spontaneous early pregnancy loss 59, possibly because these treatments don’t address other dysfunctions in the reproductive tract. This doesn’t mean that IVF causes miscarriages in PCOS patients, but rather that unmanaged PCOS reduces the success rates of IVF.
Gestational diabetes
Naturally, healthy pregnancy causes mild insulin resistance in the mother to ensure enough nutrients for the fetus. However, in women with PCOS, this mild insulin resistance may further aggravate PCOS and excess androgen. Therefore, PCOS patients are more likely to develop gestational diabetes 60.
Preeclampsia
Preeclampsia is an increase in blood pressure after the 20th week of pregnancy, followed by protein loss and edema (swelling). If left untreated, preeclampsia can turn into eclampsia, a condition with multiple organ damage and seizures. This condition occurs more frequently in PCOS patients, especially in those with insulin resistance, obesity, and gestational diabetes 61.
Preterm birth
PCOS increases the risk of preterm delivery (before 37 weeks of pregnancy)6263. Preterm infants are at risk for many health problems, both immediately post-delivery and later in life 64. Premature infants are at an increased risk of breathing difficulty, feeding problems, developmental delays, and other health issues 65. Later in life, preterm births are associated with increased risk of heart disease, diabetes, cancers, and respiratory issues 66.
Cesarean or C-section delivery
Pregnant women with PCOS are more likely to have C-sections because of the associated pregnancy complications, such as gestational diabetes or preeclampsia 67.
How PCOS is diagnosed
Many women with PCOS are completely unaware that they have PCOS, especially if they’ve always had 35+ day cycles or if their cycles are anovulatory. They may have PCOS without signs of excess androgens, and ovarian cysts without any symptoms. They only find out when faced with infertility.
It is, therefore, extremely important to have yearly check-ups with your gynecologist with ultrasound evaluation and keep a history of your menses.
PCOS is a diagnosis of exclusion because many other conditions present with a similar history, examination, and test results. To diagnose PCOS, your doctor will rule out the following conditions that present similarly in a process called “differential diagnosis” 68:
- Pregnancy as a cause of menstrual absence
- Pituitary or adrenal glands dysfunction 69. Most of the tests used to exclude them include hormone measurements and imaging techniques such as CT or MRI 70
- Thyroid disorders (read our article, linked here)
- Hyperprolactinemia (elevated prolactin)
- Nonclassical congenital adrenal hyperplasia
- Cushing syndrome
- Androgen-secreting tumors, especially if male features develop fast and suddenly 71.
Rotterdam criteria for diagnosis of PCOS
PCOS diagnosis is often delayed or misdiagnosed because it can show up differently between individuals. It also requires the exclusion of other conditions that could display similarly 72. The diagnosis of the PCOS is based on the internationally-accepted Rotterdam criteria from 2003 73. It requires at least 2 of the following 3 criteria 74:
- Menstrual irregularity – irregular (oligomenorrhea) or absent (amenorrhea) periods, and infertility
- Elevated androgens with clinical observation of hirsutism, acne, or confirmation via lab testing
- Greater than 10 follicles per ovary, as detected by vaginal ultrasound. These follicles typically occur in the periphery and resemble a string of pearls.
More recently, experts agree that polycystic ovarian syndrome is present throughout a woman’s life, even though it might not be as obvious before menarche or in menopause 75. During adolescence, PCOS features can be similar to normal pubertal development 76. Also, the diagnostic criteria could be somewhat confusing as there is no single diagnostic test, and some individual diagnostic criteria are vaguely unclear 77. Therefore, the experts are debating whether these criteria should be revised 78.
Lab tests to rule out other conditions and diagnose PCOS 79
Your doctor or endocrinologist may order the following tests to rule out other conditions and diagnose PCOS.
1) Insulin/Glucose Intolerance
- Fasting glucose/insulin ratio: <4.5 in obese, euglycemic, non-Hispanic white adult polycystic ovarian syndrome patients (<7.0 in adolescents) consistent with insulin resistance
- 75 g (4.16mmol) oral glucose tolerance test:
- Normal: 2 hour glucose <140 mg/dL (7.7mmol/l)
- Impaired glucose tolerance: 2 hour glucose 140–199 mg/dL (7.7-11.1 mmol/l)
- Diabetes: 2 hour glucose ≥200 mg/dL (11.1 mmol/l)
2) Androgens 80
Any of the following androgens may be elevated.
- Total testosterone: Levels should be between 6.0-86 ng/dl (0.21 – 2.98 nmol/L) in women. In PCOS, total testosterone may be slightly high. However, extremely high levels of total testosterone may indicate an androgen-secreting tumor.
- Free testosterone: Normal levels of free testosterone are between 0.7-3.6 pg/ mL (0.02 – 0.11 nmol/L). Free testosterone levels may be high in PCOS.
- Androstenedione: Normal levels in women are between 0.7-3.1 ng/mL (2.44-10.82 nmol/L). Elevated levels may indicate PCOS.
- Dehydroepiandrosterone sulfate (DHEA-S): Healthy levels decline with age.
- 18-19 year: 145-395 mcg/dL (3.93 – 10.72 µmol/L)
- 20 – 29 years: 65 – 380 mcg/dL (1.76 – 10.31 µmol/L)
- 30 – 39 years: 45 – 270 mcg/dL (1.22 – 7.33 µmol/L)
- 40 – 49 years: 32 – 240 mcg/dL (0.87 – 6.51 µmol/L)
- 51 -59 years: 26 to 200 mcg/dL (0.71 – 5.43 µmol/L)
3) Prolactin
Prolactin is a lactating hormone that inhibits ovulation and prevents pregnancy. 5 – 30% of PCOS patients have elevated prolactin (hyperprolactinemia), which may make it harder for them to get pregnant. In most cases, the elevated prolactin is temporary. Only 3 – 7% of hyperprolactinemic PCOS patients having persistently elevated prolactin levels. If the prolactin level does not reduce and normalize over time, your doctor may investigate other causes, such as using an MRI to rule out prolactin-secreting pituitary tumors (prolactinomas).
The normal range of prolactin is 6 – 30 ng/ml. In a study of 117 women with PCOS, 19 of them had elevated prolactin of between 30.5 – 118.2 ng/ml. The rest of the group had prolactin levels of around 15.4 ng/ml 81.
4) 17-hydroxyprogesterone
21-hydroxylase deficiency is an adrenal gland disorder caused by a genetic mutation and found in 1 in 1000 people. In people with 21-hydroxylase deficiency, steroid precursors of cortisol are converted into androgens, while all the other hormones remain very low 82. The high androgen symptoms are very similar to PCOS.
To rule out this condition, your endocrinologist will test for 17-hydroxyprogesterone from a morning fasted and without ACTH stimulation. A level of <200 ng/dL (<6 nmol/L) in the follicular phase reliably excludes this condition 83.
If levels exceed 200 ng/dL, your endocrinologist will perform a stimulated test, by injecting 250 µg of adrenocorticotropic hormone (ACTH) and then test 17-hydroxyprogesterone 30 minutes afterward. The stimulated value of ≥1,000 ng/dL (≥30 nmol/L) confirms the 21-hydroxylase deficiency diagnosis.
5) 24-hour urinary free cortisol 84
Some women with PCOS have adrenal gland disorders that result in increased urinary free cortisol and symptoms of elevated cortisol 85. Elevated cortisol can cause weight gain, insulin resistance, muscle and bone weakness, overall poor metabolic health, and blood clots 86. It is unclear whether the adrenal disorder causes the PCOS or if it is a distinct disorder.
If you have elevated urinary free cortisol and your endocrinologist suspects Cushing’s, they may order a dexamethasone suppression test. In this test, you will take 1 mg of dexamethasone at 11 PM, which is synthetic cortisol before getting your blood cortisol tested at 8 am the next day 87. In people with normal adrenals, their cortisol will be lower the next morning. Whereas in people with Cushing’s, their cortisol will remain elevated
Unlike PCOS, Cushing’s is totally curable with cortisol-reducing therapy such as radiation, surgery, or medications.
6) Luteinizing hormone/follicle stimulating hormone (LH/FSH) ratio
If you have over two times LH to FSH, you’re likely to have PCOS. However, many women with PCOS don’t have such high LH, and elevated LH to FSH is not specific to PCOS, so these two tests alone are not diagnostic of PCOS.
7) Thyroid Stimulating Hormone (TSH)
Women with PCOS may be about three times as likely to have subclinical hypothyroidism compared to women without PCOS 88. Increased thyrotrophin releasing hormone can increase prolactin and TSH, which contribute to abnormal ovarian morphology. Some women with PCOS have thyroid problems, but thyroid disorders alone can also be confused with PCOS 89. Because thyroid problems can also contribute to miscarriage, it is important to test and treat them.
The normal range for TSH, a typical test to screen for thyroid disorders is 0.3 – 4.3 mIU/L. However, for fertility and pregnancy, the American Thyroid Association recommends the optimal range of under 2.5 mIU/L 90.
8) Anti-Müllerian Hormone
If you have AMH of over 4.9 nmol/L (35 pmol/l), you may have a 92% chance of having PCOS. This test identifies 97% of women with PCOS. 91. However, because some studies have shown conflicting results, AMH levels alone may not indicate PCOS but it may be helpful in combination with the Rotterdam criteria 92.
Treatment for PCOS
The good news is that women with PCOS can manage it and maintain healthy pregnancies. In some cases, PCOS may appear to go away on its own because the natural follicle losses through the years may result in more regular cycles. In addition, most women experience subtle shortening of their cycles, with an average of 2 – 3 days between the 20s and 40s. For others, it may take multiple treatments, or even a combination between diet, lifestyle, supplementation, and medications to successfully manage PCOS.
Diet and Lifestyle modifications
Adopting healthy living habits can help reduce testosterone, hirsutism, waist circumference, fasting insulin, insulin sensitivity, and weight compared to standard treatments 9394.
Based on small clinical studies, low-carbohydrate, ketogenic diet, and intermittent fasting may help with PCOS 9596. These diets help with insulin resistance 97. A systematic review found that high-protein low-glycemic diets may be better than typical “healthy” high-carbohydrate diets for PCOS, although weight loss is beneficial regardless of diet composition 98. The clinical evidence for these diets remains limited, possibly because it is challenging to perform larger and better-controlled nutrition studies.
Dietary supplements and natural treatments
Many nutrient deficiencies are linked to PCOS or worsen PCOS symptoms. Therefore, it is important to address the deficiencies both for general health and healthy pregnancy. However, supplementation alone may not be sufficient treatment for PCOS.
Natural Insulin Sensitizers
Inositol (vitamin B8), including Myo-inositol and D-chiro-inositol, is a vitamin-like substance that can help with blood sugar control. In a small randomized-controlled trial, myoinositol helps with weight loss, several metabolic parameters, and supports ovulation 99. In a meta-analysis involving 935 women, myoinositol (4 grams) + folate (400 micrograms) showed a clear improvement of successful fertility treatments compared to folate treatment alone 100. Myoinositol is safe during pregnancy and may help with gestational diabetes 101, but we need more studies to determine whether it is effective for reducing miscarriage in PCOS women.
Lipoic acid may improve insulin sensitivity and reproductive issues according to some modest studies 102103. It lowers lipid parameters (total cholesterol). When used with myoinositol, it can reduce insulin and androgen hormone levels 104105.
Folate
Many women with PCOS who suffer from multiple miscarriages are more likely to have high homocysteine. High homocysteine can cause miscarriage and pregnancy complications. There are many potential causes of elevated homocysteine, including folate deficiency, MTHFR mutations, thyroid disorders, and kidney issues 106107. Among women with PCOS and elevated homocysteine, taking folate seems to help them achieve successful pregnancies 108.
Vitamin D, Calcium, and Magnesium
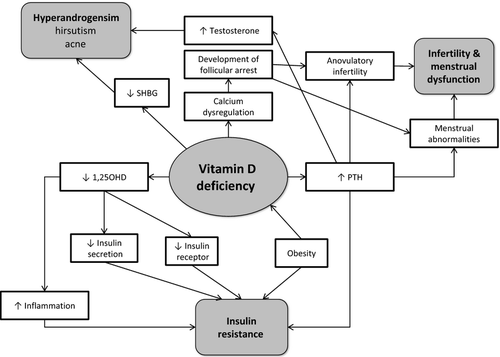
Vitamin D deficiency (25(OH)D<20 ng/ml) is found in 67 – 85% of women with PCOS. Possibly, suboptimal vitamin D levels (<30 ng/ml) may be even more common 110. A genetic variant in the VDR gene correlates with the severity of PCOS but not disease risk itself 111. In addition, vitamin D deficiency is linked to many metabolic and inflammation hallmarks of PCOS. Sensibly, a systematic analysis of randomized controlled trials found that up to 4000 IU/day of vitamin D helps with insulin sensitivity in PCOS patients 112. Another meta-analysis found that it helps with body mass index, DHEA-S, triglycerides, and increasing HDL cholesterol 113. Vitamin D supplementation also has been shown to help reduce endometrial thickness and TGF-β1, a marker of PCOS severity 114115. Therefore, correcting vitamin D deficiency is clearly beneficial for PCOS patients. Read more about Vitamin D, linked here.
Vitamin D works with calcium and magnesium, so it may be beneficial to take all three of them for PCOS. Magnesium deficiency is very common and most people don’t get the recommended daily allowance levels (300 – 400 mg) in their diet. The deficiency can contribute to insulin resistance and pregnancy complications, so correcting a magnesium deficiency can be beneficial.
Thus far, clinical trials of magnesium in PCOS have been mixed, suggesting that magnesium alone may not be sufficient or that there are more individual factors at play 116.
In a small clinical study of 100 women, 1000 mg calcium and 100,000 IU/month of vitamin D combined with metformin for 6 months significantly helped with weight loss compared to metformin alone. In addition, this vitamin D and calcium regimen group also had somewhat improved menstrual regularity, better follicle maturation, and fertility 117. Another study also observed similar benefits with 6000 IU of vitamin D, 1000 mg calcium, and 1500 mg of metformin compared to metformin plus placebo 118.
Omega-3 fats
In the general population, the omega-6 to omega-3 ratio is often higher than optimal. This contributes to metabolic and inflammatory diseases 119. For PCOS patients, omega-3 fatty acid improves insulin resistance and blood lipids 120.
Other natural treatments
Quality of life in women with PCOS can be improved with exercise and acupuncture 121122. Yoga may also help with testosterone levels in PCOS 123.
Medications
These medications are typically prescribed as first-line therapy for PCOS, including during the preconception period and discontinued in pregnancy.
Hormonal contraceptives
Intermittent progestin (medroxyprogesterone 5 to 10 mg orally once a day for 10 to 14 days every 1 to 2 months) or oral contraceptives are first-line therapy to regulate menstrual cycles and reduce androgens. These drugs may also help insulin resistance and improve the control of LH and FSH 124.
Metformin
At 500 to 1000 mg twice a day, metformin increases insulin sensitivity in women with PCOS if lifestyle modifications are ineffective. Metformin can also reduce free testosterone levels, make cycles more regular, and induce ovulation. The doctor may recommend a contraception method for couples who don’t desire pregnancy. Metformin may also improve live birth rates compared to placebo despite some digestive side effects 125.
Clomiphene
Many women with PCOS have irregular cycles or no ovulation. Clomiphene (Clomid) induces oocyte maturation and ovulation by triggering a huge burst of FSH and LH. After ovulation, progesterone and estradiol rise and fall like they do in a normal ovulatory cycle. Clomid is a selective estrogen receptor modulator, with both estrogenic and anti-estrogenic properties. For women who desire pregnancy, clomiphene is the first-line therapy for infertility. Clomiphene can lead to multiple ovulations, which increases the risk of conceiving twins. It is given orally at 50 mg daily, for around 5 days, starting from day 5 of your cycle.
Things to keep in mind when about clomiphene
When using ovulation-stimulating drugs like clomiphene, your doctor may instruct you to follow your ovulation with an ovulation predictor kit. It measures LH surge in your urine sample to help you plan intercourse. The optimal timing of intercourse is on the day of the LH surge and one day after. Alternatively, the couple is advised to have intercourse every other day for one week, beginning around day 10 of the menstrual cycle. The doctor may also recommend a transvaginal ultrasound to evaluate the size and number of developing follicles.
Conclusion:
Having PCOS can seem scary with many unknowns, but you are not alone and many women with PCOS have had successful pregnancies. If you have symptoms of PCOS, it is important to work with your doctor and ensure that you get the correct diagnosis. If you have been diagnosed with PCOS, much of the diet, lifestyle, and supplementation options are safe and effective ways to manage PCOS. You also want to monitor your homocysteine, PAI-1, vitamin D, and thyroid hormone levels because these factors are associated with miscarriage in women with PCOS. Lastly, prescription medications as well as natural treatments for blood sugar management, ovulation induction, and fertility treatments may also be helpful.
Next Steps to Consider
- If you have been diagnosed with PCOS, discuss the above lifestyle, diet and other treatment options with your doctor
- If you think you might have PCOS, find a doctor or other health professional that specializes in working with women with PCOS who can help with a diagnosis and treatment options
- Stay hopeful! Women diagnosed with PCOS can go on to have a successful pregnancy.
References

0 Comments